
NZNO Kaiwhakahaere Kerri Nuku and I were honoured and deeply humbled to be the Chief Guests at the 61st AGM of the Fiji Nursing Association (FNA), held in Suva on 28 April 2018. It was the first time that elected NZNO leaders had been formally invited to Fiji. Our invitation reflected decades of work with the FNA by many people in our organisation. I spoke second, after the Kaiwhakahaere, and delivered this speech.
Ni sa bula vinaka, kia ora koutou, warm Pacific greetings to you all.
It is customary in our country, when beginning a formal speech at a meeting, to start by acknowledging the Creator, and those who have gone before as well as those present. This custom has been adopted from the indigenous culture of Aotearoa New Zealand. Over the last two days I have been learning of the many similarities between this Māori culture and the cultures of Fiji.
Nō reira, Ko te kupu tuatahi, ki to tātou kaihanga, nāna nei te kākano i ruia mai i Rangiātea.
E ngā mate, haere, haere, haere. Rātou te hunga mate ki a rātou. Tātou te hunga ora e huihui mai nei, tēnā tātou.
To translate: my first word was to the Creator, who sowed the seed from the realm of beginnings, and endings. I greet those who have passed on, and the living assembled here.
To introduce oneself, we speak of the place and the people we belong to. We refer to our connection to the natural and spiritual world of our birthplace, to a shared experience of migration and to a collective identity based on ancestry – as Kerri also did, a few moments ago.
Ko wai ahau?
Ko Kapukataumahaka tōku maunga
Ko Owheo tōku awa
Ko Cornwall tōku waka
Ko te Tāngata Tiriti tōku iwi
Ko Grant Brookes taku ingoa, ā, ko te perehitene ahau ō te Tōpūtanga Tapuhi Kaitaiki ō Aotearoa.
Who am I? The sacred mountain overlooking my birthplace is Kapukataumahaka, and the sacred river is Ōwheo. My ancestors arrived on board the ship, Cornwall. My tribe is known as the People of the Treaty, which means I am not indigenous. I reside on the land by right of Te Tiriti o Waitangi, the 177-year old treaty between the Māori peoples and the British Crown. My name is Grant Brookes and I am the Co-President of the New Zealand Nurses Organisation Tōpūtanga Tapuhi Kaitaiki ō Aotearoa.
Our bicultural leadership model, reflecting Te Tiriti, consists of indigenous and non-indigenous Co-Presidents. Kerri, who has just spoken, is the other Co-President of NZNO. Her Māori title is Kaiwhakahaere.
In a formal speech it is then customary to pay respects to the land on which we are meeting and to its traditional guardians. So, as a vulagi, I acknowledge the vanua, the people of the Burebasaga confederacy and the ancestor Ro Melasiga, or Ro Koratu.
Vakaturaga i Kubuna, Burebasaga, Tovata.
I acknowledge also ngā rau rangatira mā, the many great nursing leaders from Fiji and around the Pacific I see before me, and I thank Dr Adi Alisi Vudiniabola and the Fiji Nursing Association for the invitation to speak today.
I am here with you at an historic time for nurses, midwives and health care assistants in Aotearoa New Zealand.
Six days ago, on Monday, the 28,000 members of NZNO who work in the public health system, for our District Health Boards (DHBs), began voting to strike.
It is just the fifth time in the 109-year history of our organisation that such a vote has been held.
The last time that NZNO members in the public health system voted to strike was part of a famous episode in our history – an episode which also marked the beginning of stronger bonds between our organisation and yours.
The year was 2004, and our claim was for a single, multi-employer collective agreement (MECA) to unite all of our members in the DHBs, for safe staffing levels, and for pay equity with teachers and police. This would mean pay increases of between 20 and 47 percent – the biggest ever seen in New Zealand’s public health system until that time.
We called it our “Fair Pay campaign”, and it was successful.
In February 2005, as our celebrations were about to get under way, we were privileged to receive a two-week long visit from Pacific nursing unionists, including Miriama Vakaloloma and your current Vice-President, Miliakere Nasorovakawalu. The story is told in the pages of our NZNO journal, Kai Tiaki Nursing New Zealand.

Afterwards, the leaders of our NZNO Fair Pay campaign, Laila Harré and Lyndy McIntyre, came to Fiji to meet with FNA members.
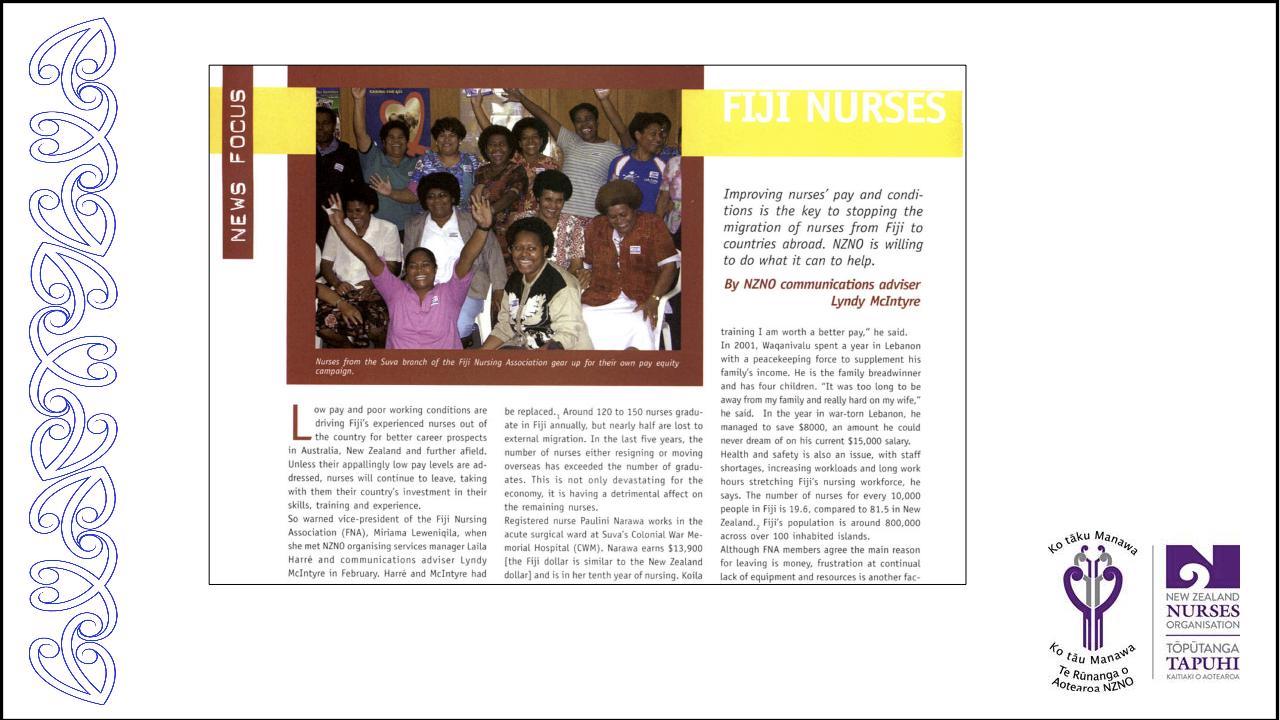
When on International Women’s Day, 8 March 2005, the FNA launched your own Fair Pay campaign, it was a great honour for us. We were pleased to be able to share the fruits of our work, sending Fair Pay stickers and t-shirts, and to see how you were able to improve on our campaign tactics. To win support for your campaign, you produced postcards for people to send to the politicians – like ours, but with the addition of a prayer on the back.
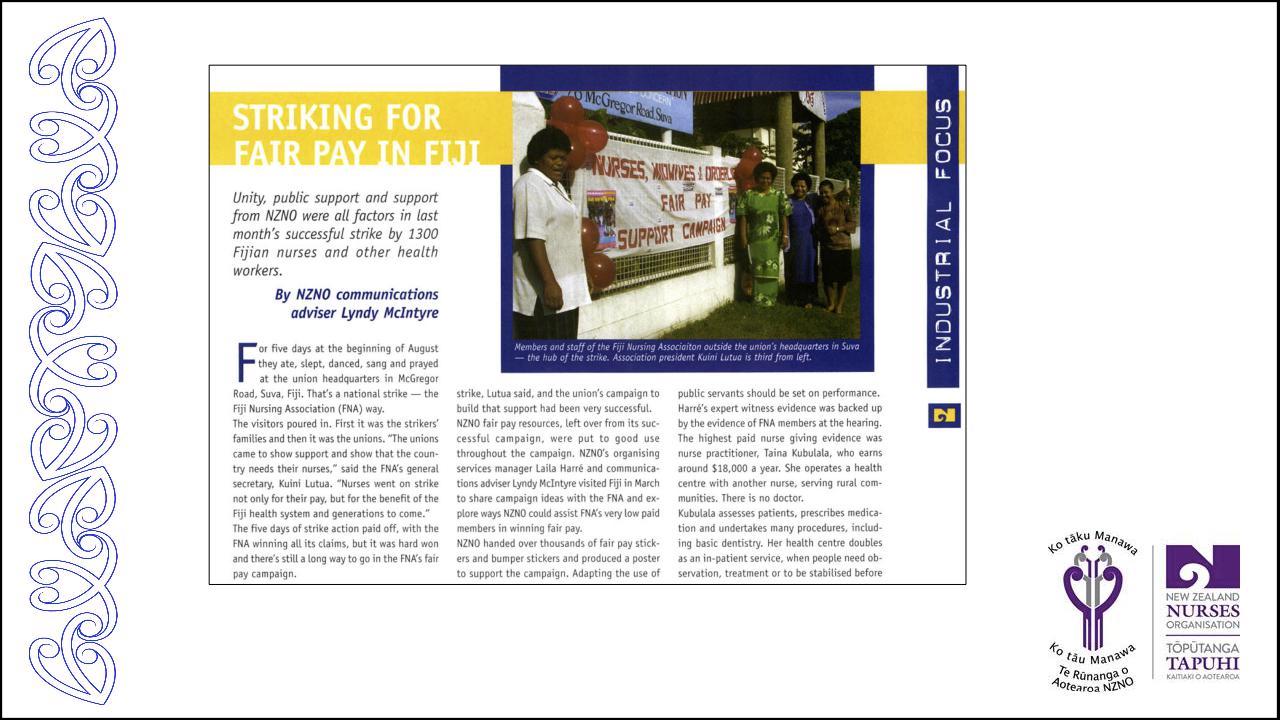
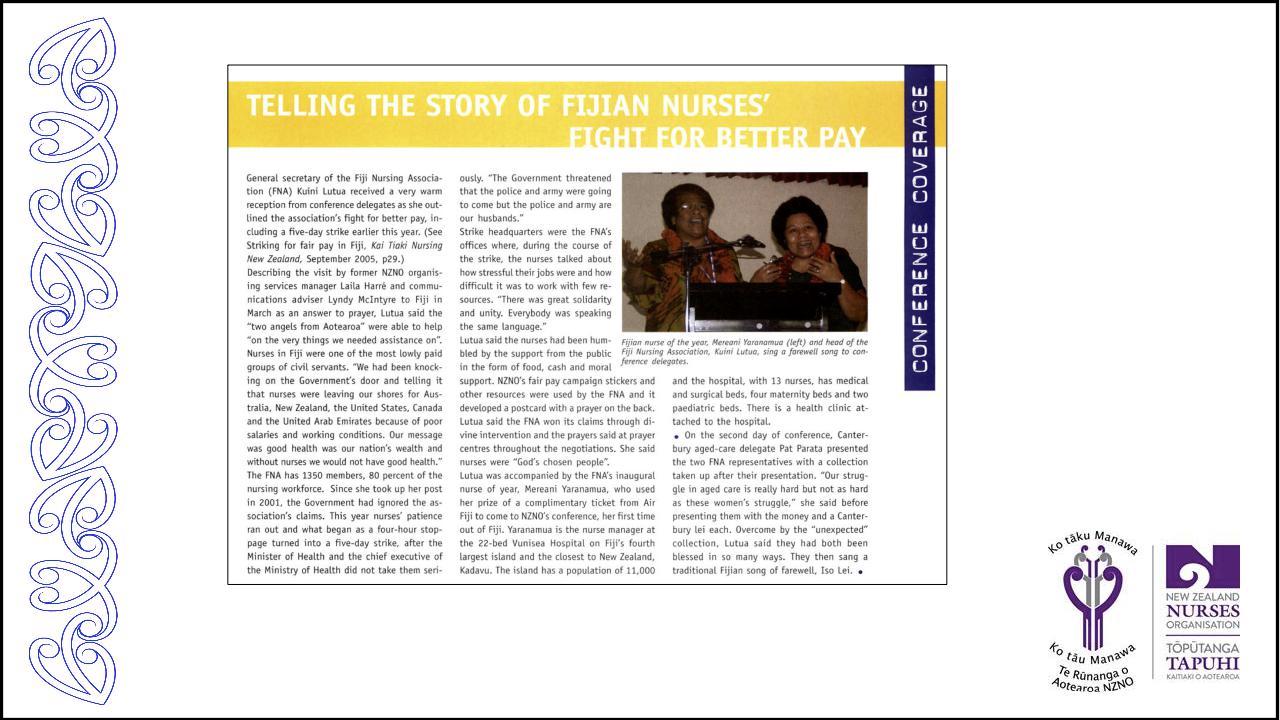
Laila Harré also gave evidence at the arbitration hearing here in Fiji against performance pay for nurses. After your successful five-day strike in August, your general secretary Kuini Kutua and Nurse of the Year Mereani Yaranamua were guests of honour at our 2005 NZNO AGM and Conference. The inspiration they brought to New Zealand was immeasurable.
Two years later, our NZNO chief executive Geoff Annals was able to reciprocate, attending your 2007 FNA AGM.
Later in 2007, we watched avidly as nurses and midwives in Fiji again took industrial action – this time, for 17 days – to stop a five percent pay cut. The NZNO Board of Directors was able to return Kuini’s and Mereani’s gift and make a small contribution to support FNA members facing hardship. When you won, we also celebrated your victory for nurses and patients.
In 2008 we were again here with you in Fiji, when the FNA hosted the 14th South Pacific Nurses Forum.

Kuini and 30 FNA members came to Auckland for the next Forum in to 2010.

More recently, NZNO members volunteered to join the New Zealand Medical Assistance Team which was deployed to Fiji in the aftermath of Cyclone Winston.
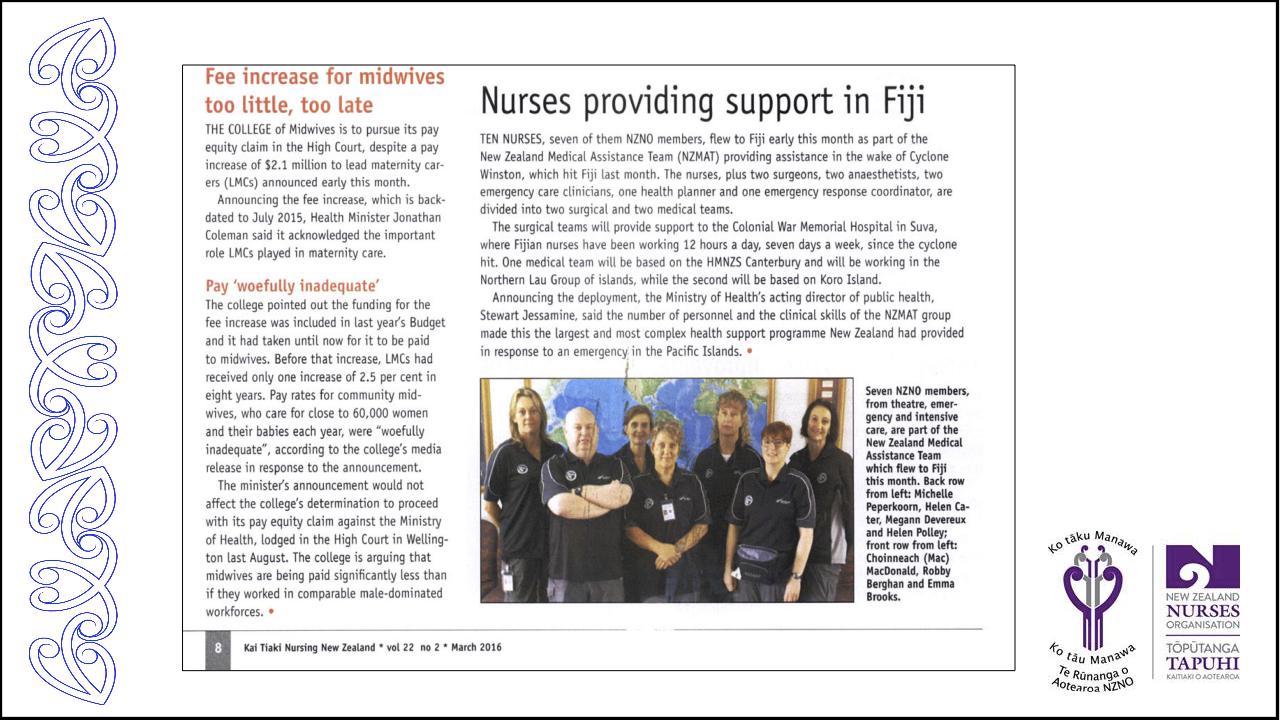
My friend and colleague from Wellington Hospital, Emma Brooks (second from right in the photo), sent back amazing stories of extraordinary and outstanding service by Fijian nurses to their communities, some of which had been almost devastated by the cyclone. Seeing the humanitarian need, the NZNO Board had to respond with support for the FNA.
And last year, we welcomed the chance to work with our sister union, the New South Wales Nurses and Midwives Association, on your FNA submission about the new pay structure for nurses and midwives.
Our stories, as Fijian and New Zealand nurses and midwives, as Pacific trade unionists, are intertwined. Our bonds of friendship and solidarity are many and strong.
And so it continues, as we now embark on fresh campaigns for health as a human right.
“Nurses: a voice to lead – health is a human right” is the theme for this FNA Symposium and AGM. It is also the theme set by the International Council of Nurses for International Nurses’ Day (IND) this year. As Dr Adi Alisi has just mentioned, the idea of health as a human right is not a new one. It is an idea which guides our work as NZNO – including the ballot on strike action in the DHBs which started last Monday.
In her introduction to the IND information kit, ICN President Annette Kennedy says individuals and communities all over the world are suffering from illness due to a lack of accessible and affordable health care. But nurses also need to remember that the right to health applies to us as well.
“We know that improved quality and safety for patients depends on positive working environments for staff”, she says. “That means the right to a safe working environment, adequate remuneration, and access to resources, and education. We must add to this the right to be heard and have a voice in decision-making and policy development implementation.”
The right to health is underpinned by national and international legal instruments and conventions, such as Section 38 of the Fiji Constitution or the third of the United Nations Sustainable Development Goals (SDGs). SDG3 sets the target of achieving Universal Health Coverage by the year 2030.
And what is Universal Health Coverage? According to the World Health Organisation, “UHC means that all individuals and communities receive the health services they need without suffering financial hardship. It includes the full spectrum of essential, quality health services, from health promotion to prevention, treatment, rehabilitation, and palliative care.”
At the pre-AGM Symposium held on Thursday and Friday, there was a focus on how far there is to go for Fiji to reach this goal. My country, on the other hand, is generally thought to have achieved this target long ago, as far back as the end of the 1930s. But is this really so? Do we have Universal Health Coverage in New Zealand today?
Surprisingly perhaps, the New Zealand government does not collect and publish comprehensive data showing whether individuals and communities receive the full spectrum of health services they need without suffering financial hardship. Without this data, you might ask, how can we report on our achievement of Universal Health Coverage? How can we identify priority areas for attention?
But a few measures of access and barriers to health services are contained in the New Zealand Health Survey, conducted annually by the Ministry of Health. The results for the 2016/17 year, published in December, include some disturbing findings, such as:
- 28 percent of New Zealand adults reported trouble getting seen in primary care
- 1 in 7 adults (14 percent) reported not visiting a GP due to cost in the past year.
- Less than half of adults with natural teeth (47 percent) visited a dental health care worker in the past year
- 268,000 adults (seven percent) reported not collecting a prescription due to cost in the past year.
The International Health Policy Survey, conducted by the US-based Commonwealth Fund, is another source containing some measures of access to health services for individuals and communities.
In the latest survey, New Zealand ranks poorly against similar countries for access-related performance measures, in particular access to diagnostic tests, long waits for treatment after diagnosis, long waits to see a specialist and long waits for elective surgery.
Of the New Zealand doctors surveyed, 59 percent reported difficulty in gaining access to diagnostic tests for their patients, and 34 percent said patients “often experience long waits to receive treatment after diagnosis”. Twenty-one percent of New Zealanders surveyed reported cost-related barriers to accessing health care.
The lack of comprehensive New Zealand government data on unmet health need last year led a group of medical researchers to conduct a pilot study. Their research, published in the New Zealand Medical Journal, found at least 25 percent of adults were unable to get the primary health care they required while 9 percent of people had unmet secondary health care needs.
Christchurch surgeon Dr Phil Bagshaw, one of the lead authors, said, “There are probably hundreds of thousands of people who have an unmet need that are not recorded”.
Bagshaw said the 9 percent of people with an unmet secondary health care need in the survey had been told by a specialist they needed treatment but had not received it, generally because they didn’t meet the criteria to go on the waiting list.
The major reason for this emerging picture that human rights to health and Universal Health Coverage are under serious threat in New Zealand is nine years of cumulative health underfunding. Government spending on health has failed to keep pace with population and cost increases each year since 2009/10. It has also fallen as a percentage of GDP. Each year, health spending has slipped further and further behind. In the current financial year, the shortfall compared to 2010 reached $1.4 billion.
The impact is being felt not only by the individuals and communities who are unable to receive the full spectrum of health services they need without suffering financial hardship. It is also being felt by nurses, midwives and health care assistants working in the public health system.
Over the last decade, the underfunding of our public health services has meant that NZNO members have reported ever-increasing workloads, increasing patient acuity (patients are sicker coming into hospital), stress, fatigue, and lack of job satisfaction. This is contributing to high staff turnover and to lower morale. Our members are also impacted by inadequate levels of staffing, unhealthy shift rostering, the undervaluation of nurses work and a lack of appropriate access to continuing professional development and study leave.
Which brings us back to my starting point. I am here with you at an historic time for nurses, midwives and health care assistants in Aotearoa New Zealand. For the first time since 2004, the 28,000 members of NZNO who work in the public health system, for our DHBs, are voting on strike action.
The vote is the latest step in our new campaign. This one is called #HealthNeedsNursing.
Health Needs Nursing has a dual message. On the one hand, it is an affirmation that the nursing team is the essential core of the health system. We are dedicated, caring and always there.
Health Needs Nursing also says that the health system itself is sick. It too needs to be nursed back to health.
The goal of our campaign is to rebuild our public health system back to good health. The immediate staffing crisis has to be addressed. Full employment of new graduate nurses and employment of additional nurses to achieve the right skill mix matched to the needs of patients is required for New Zealand to truly claim Universal Health Coverage. Our goal is to enable nurses to maintain a standard of care that equates to our professional standards – a standard patients deserve.
Equally, our members salary structure does not adequately recognise experienced staff nor does it incentivise nurses to remain in the profession. Inadequate pay is contributing to a vicious cycle of high nursing staff turnover. Investment in fair pay for our DHB MECA nursing and midwifery teams is urgently required.
Over the last three weeks, thousands and thousands of NZNO members and supporters have taken action, from one end of the country to the other, in the big cities and in the small towns, too.

There have been at least 34 rallies for good health held so far – the latest one at Burwood Hospital in Christchurch just yesterday.

You may recognise some of these faces. In the photo on the top right is Christchurch nurse Simione Tagicakibau, who presented at the FNA Symposium yesterday on Pacific health models in New Zealand.
We’ve been front page news.

We’ve been on TV, too. Click on the image to watch the news story.

We are not just protesting, though. We are also engaging with members of the public at markets and public transport hubs, talking with them about the need to rebuild our health system. These photos were taken at Wellington Railway Station.

We are sending thousands of electronic postcards to government ministers. We are collecting stories from our members to submit to an independent panel which is considering ideas for resolving the dispute.
And we are winning. On Tuesday, Prime Minister Jacinda Ardern said that the government is factoring our claims into the way it is working up its Budget, due to be released on 17 May.
We are hopeful that our goals can be achieved without resorting to industrial action. If strikes do go ahead, they are scheduled for early July.
But to ensure health as a human right in Aotearoa New Zealand, it will take more than a win for our #healthneedsnursing campaign.
Discussion at the FNA Symposium over the last two days has highlighted the lack of health equity between countries, such as Fiji on the one hand and Australia and New Zealand on the other. Achieving the UN Sustainable Development Goals means reducing this health inequity. NZNO is committed to multilateral cooperation in advancing global health equity and addressing global health crises and risks.
At the same time, it is important to address health disparities within countries, including within New Zealand, which undermine any claims of Universal Health Coverage.
Earlier this year, New Zealand reported on progress against another UN framework, the International Covenant on Economic, Social and Cultural Rights. The UN committee responsible for overseeing the convention looked at outcomes in a range of areas such as health, housing, education and employment. According to Janet Anderson-Bidois, chief legal adviser/tumuaki kaitohu ture at the New ZeaLand Human Rights Commission/Te Kahui Tika Tangata, the committee expressed surprise and concern about the information it received from the government, and in separate reports provided by the Human Rights Commission (HRC), NGOs and community groups.
“The reports revealed significant disparities in key health areas for groups such as Māori, Pacific people, disabled people and the LGBTI community”, said Janet Anderson-Bidois. “Māori and Pasifika are more likely to be affected by preventable conditions, and to die prematurely. They have a greater chance of experiencing mental illness, dying at work or committing suicide.”
In order to reduce these disparities and ensure health as a human right for all, it is necessary to strengthen culturally appropriate services and workforce. For this reason, alongside our #HealthNeedsNursing campaign in the DHBs, NZNO is also campaigning for equitable funding for Māori and Iwi (or tribal) health providers, for a pay parity for nurses working in these providers with their DHB colleagues and for a doubling of the proportion of Māori nurses, to match the population. This NZNO campaign is being led by Kerri Nuku and our Māori governance group, Te Poari o Te Rūnanga o Aotearoa NZNO.
Following in the footsteps of Whina Cooper who we have just heard about, Kerri led a Hīkoi (or peaceful march) in 2016 from the Te Puea Memorial Marae in Auckland to the Indigenous Nurses Aotearoa Conference.

The hīkoi was a show of collectivism, solidarity, enabling members of Te Rūnanga to kōrero, to waiata, to celebrate and to advocate for pay parity for Māori and Iwi Provider nurses.
In conclusion, I hope that these stories from NZNO stimulate your discussions today, and in times to come. I believe they show how FNA and NZNO have worked together over the years, in bonds of solidarity and Pacific friendship, and how we can continue to walk our paths together in future.
Finally, to conclude a formal speech in the custom of the indigenous people of Aotearoa, we greet three times the people gathered at the meeting.
Nō reira, tēnā koutou, tēnā koutou, tēnā tātou katoa.
Vinaka vakalevu

One thought on “‘Walking together in solidarity & Pacific friendship’ – Speech to Fijian Nursing Association AGM”