
(Following some unscripted remarks on the events in Christchurch the previous day, these were the speaking notes for my presentation.)

Āta mārie, tēnei te mihi ki a koutou.
Good morning, greetings to you.
Ko wai ahau? Ko Kapukataumahaka tōku maunga, ko Ōwheo tōku awa, ko Cornwall tōku waka.
Ko te Tāngata Tiriti tōku iwi, ko Don rāua ko Helen ōku mātua. Ko Grant Brookes ahau. Nō reira, tēnā koutou katoa.
Who am I? The place I come from looks up at a mountain called Kapukataumahaka, or Mount Cargill, and sits beside a river called Ōwheo, the Water of Leith. My ancestors arrived there, in Dunedin, aboard a waka, or ship called The Cornwall. I belong to the People of the Treaty, the people who reside here under the agreement first signed at Waitangi in 1840. My parents are Don and Helen, and I am Grant Brookes.
The topic I have been given to speak about is, “Where to from here? Into the future, the path forward, what is the role for migrant nurses in NZNO?”.
Let’s begin with definitions. What is this group, the migrant nurses in NZNO? Who are they?
The answer may surprise you. We don’t entirely know.
The NZNO membership database contains a field recording a member’s “country of first qualification”. In theory, therefore, the migrant nurses in NZNO should be clearly identifiable. They would be the members who ticked a box other than “New Zealand” in their membership application, in response to this question.
However, in speaking with the NZNO Membership Department in preparation for this talk, I learnt that it’s not so simple.
Firstly, this field was added to the database only around four years ago. For members who joined prior to that, there is no record of where they first qualified. And I was told that anecdotally, the data is not reliable, as many members who have joined since 2015 left this field blank on their membership form, or filled it out incorrectly.
But when we speak of migrant nurses (and of internationally qualified health workers who may not be working as nurses, the other group covered by this conference), what we’re often thinking of are people who share particular cultural backgrounds – backgrounds other than New Zealand European or New Zealand Māori. Research suggests that the experiences of NZNO members in these minority groups (including experiences of racism) are similar, regardless of whether the person first qualified as a nurse in New Zealand or overseas.
In other words, what we’re talking about is ethnicity. And with your permission, I would like to focus on this concept, which thankfully is captured by NZNO in a time-series data set which is more robust.
Do you like data? I do, as you may have guessed. So if you’re not a fan, please indulge me for a couple of minutes as I present some charts showing the changing ethnic makeup of our membership over the last ten years.
Just one final word about data quality – up until 2015, ethnicity categories in the NZNO membership database were less specific. So, for example, members belonging to one of the many Asian ethnic groups were described as either Chinese, Indian or “Other Asian”. The NZNO Board requested refinements to the reporting categories in 2016, to make the growing diversity of our membership more visible. You will see this in the later charts. Ethnicity data captured in the NZNO database is now aligned with the fields recorded by the Nursing Council, although it’s still not perfect and anecdotal reports suggest a member’s ethnicity sometimes defaults incorrectly to NZ European.
So based on what we have, this was the picture at 31 December 2008.
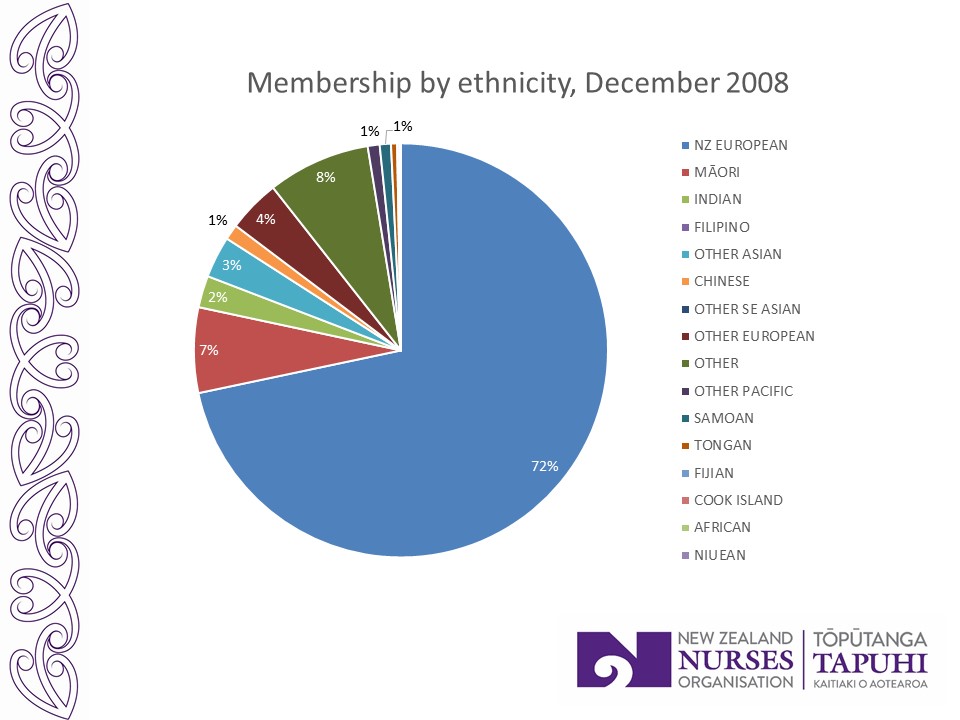
Our membership was largely made up of people identifying as New Zealand European, with a significant Māori group. There was also a visible group of “Other Europeans”, reflecting the traditional trickle of migrant nurses from places like the UK and Australia.
Click on the image to play the video below and watch how it changes, year by year.

In 2010, the “Other Asian” group started to overtake “Other European”, as the primary source countries for IQNs started to change. The trend then accelerated.
And this is where we are now.
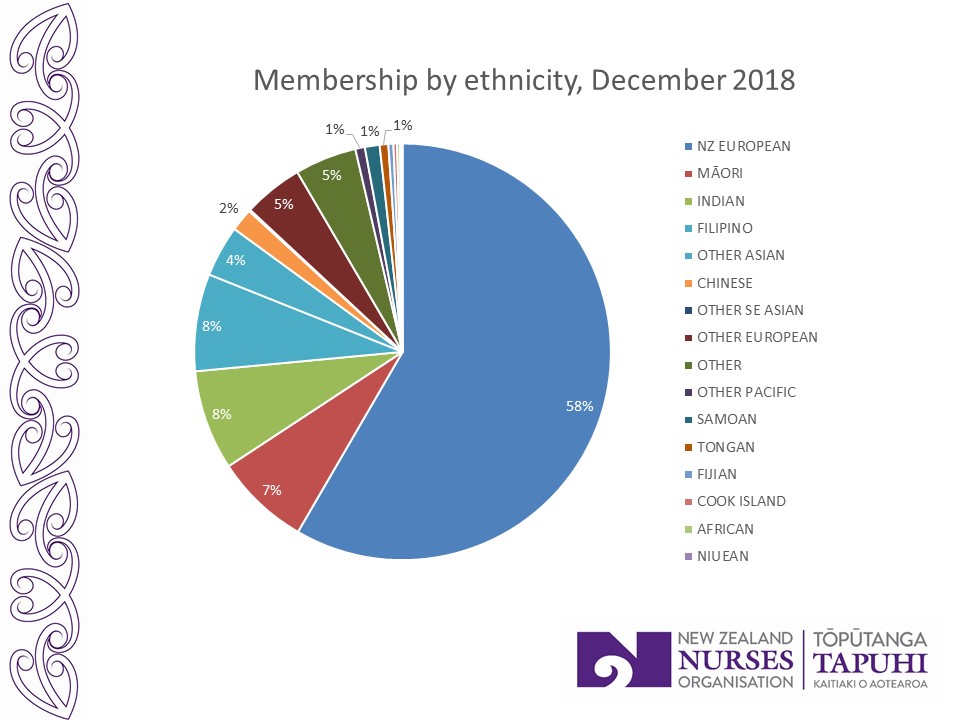
If current trends continue, New Zealand Europeans like me will be a minority of NZNO members by 2025.
It is worth mentioning in passing that there hasn’t been any similar transformation of the NZNO staff. There are almost 130 people employed by NZNO, in a variety of roles. But aside from our Chief Executive, there are still no IQNs of non-European ethnicity among them.
So that’s the picture from the last ten years. But if you go back further, the demographic transformation of the NZNO membership appears starker still. I became a member of NZNO in 2002. Back then, the organisation looked like this.

As you can see, the NZNO which I joined was largely monocultural, at least as far as our membership base was concerned.
You might also note that the opening up of this monoculturalism has come through the declining proportion of members identifying as New Zealand European. Māori membership has not declined. The proportion of members who are tāngata whenua, or people of the land, and the proportion who are tauiwi, or more recent arrivals residing here by virtue of Te Tiriti o Waitangi, is virtually unchanged through this period.

The relationship between these two groups underpins the bicultural foundation of our organisation – in accordance with the bicultural foundation of our nursing profession, and indeed of our nation. Kerri Nuku will speak more about this next.
If this is the story so far, what is the role for IQNs and migrant health workers in NZNO, into the future?
Let me first flip that question. What is my role, as Co-chair of the NZNO Board, for IQNs and migrant health workers in NZNO?
I know that as a New Zealand European, citizen and NZRN, I automatically benefit from a system of privilege, whether I like it or not. My role for IQNs and migrant health workers in NZNO is to use that privilege to make space at the top table for people without it, like you.
Your role is quite simply to take your place in the leadership of NZNO – as increasing numbers of you are already doing.
I would like to briefly showcase just a few of the leading roles being filled by migrant nurses today. Some of these people, you will probably recognise.

Victoria Santos is an IQN from the Philippines. She also holds a senior leadership position in the governance of NZNO. Victoria sits on the Membership Committee, the national body which advises the NZNO Board of Directors on the views and needs of the diverse membership. The Membership Committee also helps to carry out delegated work such as drafting the constitutional changes which will this year see voting on NZNO policies and rules opened up to everyone, though an online “one member, one vote” system.

Jed Montayre is also from the Philippines. Within NZNO, Jed is an elected member of the National Committees of Gerontology Section and also the Nursing Research Section. He has served on the abstracts committee which selected the papers for presentation at the NZNO Annual Conference. Here, he is pictured receiving the award as joint winner of the NZNO Young Nurse of the Year in 2016.
One of the three abstracts chosen for last year’s NZNO Annual Conference was on “The Experience of Migrant Health Workers in New Zealand”. It was jointly presented by three Filipinos – Joey Domdom, Judith Salamat and Mayie Pagalilauan – in conjunction with Toga Katyamaenza, an IQN from Zimbabwe. Here they are pictured with IQN and former NZNO Board member Monina Hernandez, who will speak to us later this morning.


Shamim Chagani is an IQN from Pakistan, and an elected member of the National Committee for NZNO Nurse Managers New Zealand. She is also the editor of the Nurse Managers’ newsletter, Te Wheke, a Māori title which means, “The Octopus”.
But IQNs are not just demonstrating professional leadership within NZNO.

This poster features Ebson Abraham, an IQN from India. The poster was produced by the NZNO Tai Tokerau Regional Council for International Nurses Day last year, to celebrate local NZNO leadership in Northland. The writing is probably too small for you to read, but it says Ebson was a workplace delegate at Cairnfield House Rest Home in Whangarei, where “he took responsibility for NZNO services, promoting the union movement from scratch and then constructed a movement that is measurable by the increase of NZNO membership density up to 80% that eventually built a strong force for change. This wave became a pillar… for NZNO bargaining in 2016/17 with an effective settlement of a collective agreement in 2017”.
As an aside, there is a widespread assumption among New Zealanders that union membership and activism are somehow foreign to the cultural values in the primary source countries for IQNs today.
The diversity clearly displayed on marches and rallies by DHB nurses last year should help to dispel that stereotype. But so would greater knowledge of overseas nursing unions, which are growing under very difficult conditions and waging struggles on a scale and intensity which make our DHB strike look timid.
A case in point is the United Nurses Association of India. It was formed in the southern state of Kerala in 2011, in response to the suicide of a nurse who had been bullied by her managers. It now numbers over half a million members. Months of protests and strikes in 2017 and 2018 won agreements on pay rises for around 80,000 nurses in private hospitals. At one hospital in Kerala, nurses remained on strike and picketed outside the facility daily, for over a year.
The spectacular rise of the United Nurses Association is an amazing story. I hope to meet leaders of that union for the first time in July at the annual meeting of our international union federation, Global Nurses United. But it’s by no means an isolated case. Nurses in the Philippines have been organising for decades – again under very difficult conditions – through unions including the Alliance of Health Workers and more recently through Filipino Nurses United. Last year, Kerri Nuku and I attended 61st annual general meeting of the Fijian Nursing Association. FNA has been active as a Pacific nursing union since 1977, including campaigning for workers’ rights under military rule, and so on.
Returning to the slides, the last two IQN leaders in NZNO I wish to showcase highlight the need to avoid assumptions when it comes to migrant nurses.

Current Board member Eseta Finau occupies the highest leadership role in NZNO of any IQN. She will talk to us shortly about that role. Despite also being the most Tongan person I know, however, she actually qualified as a nurse in Australia. Gidday cobber!
And then there are NZNO leaders who you might not pick as IQNs from their appearance.

Debbie O’Donoghue is a former NZNO Board member who now serves on the national committee of NZNO Nurse Managers New Zealand. She is also an IQN, from the UK.
But leadership for IQNs within NZNO does not depend on holding a title, like these people. The NZNO Strategy for Nursing 2018-2023 recognises that, “Many nurses demonstrate excellent… leadership, though they may not recognise this, associating leadership only with formal roles.”
In many ways, leadership exercised by people without a formal title is the most important kind. As Bernie Sanders likes to say, “Real change does not happen from the top down. It happens from the bottom up.”
One of the ways that any member can influence NZNO’s direction from the bottom up is by responding to consultation requests. This is where staff from the NZNO policy and research team seek member input, in order to determine NZNO’s position on a wide range of issues. They do this by emailing all member groups, including Regional Councils, to ask for feedback.
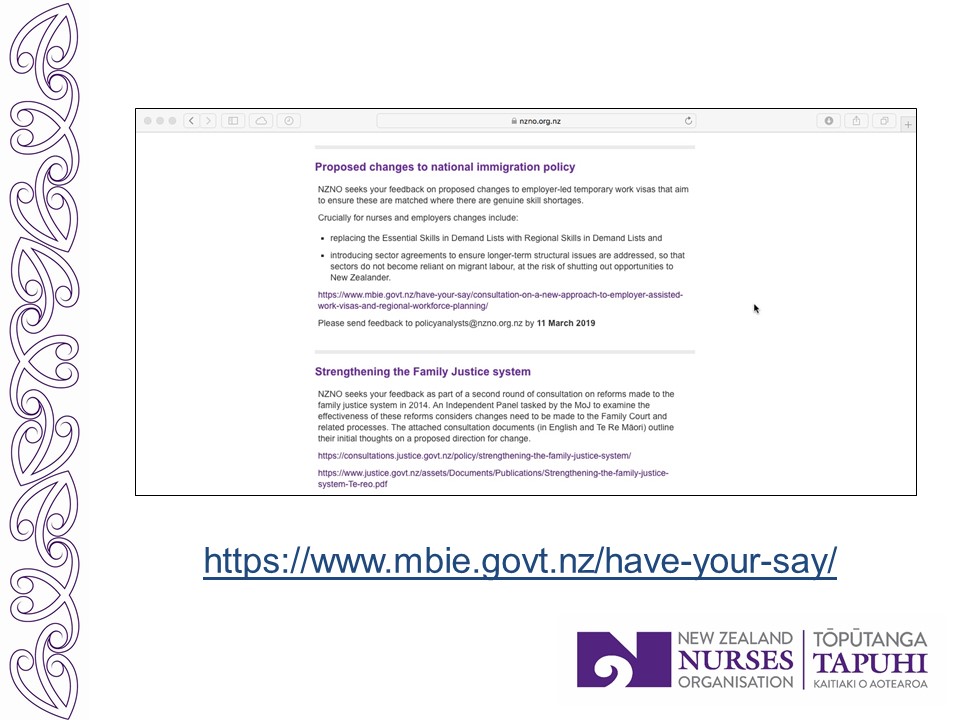
They also post the requests on the NZNO website, under the menu “Get Involved > Consultation”. If migrant nurses are not getting the consultation requests by email, from a member group, you can sign up on the website to be notified each time a new one comes out.

Here is a recent request, asking for input to shape NZNO’s view about the changes to temporary work visas for migrants currently being proposed by the government. Unfortunately, the deadline has passed for people to respond to this request, although if anyone is interested in making an individual submission to the government, you can do it via the MBIE website until Monday, at the address on screen.
So these are some of the ways that migrant nurses can take up your role as leaders of NZNO and use your power to make a difference.
But as the title of Monina Hernandez’s presentation on today’s programme reminds us, the role for migrant nurses in NZNO is not just about “making a difference”. It’s also about “being yourself”. I will end on this point.
Coming up before morning tea is Abel Smith’s presentation, “An introduction to the Pacific Nursing Section”. The PNS is one of NZNO’s 20 colleges and sections. I am really looking forward to it because for me, this group epitomises what it means for ethnic minority members to be themselves while also making a difference.
NZNO sections and colleges are groups of members with a focus on a specific field of nursing. The colleges are groups relating to a specific clinical specialty, while the sections are groups representing a role or membership classification, such as those sharing a specific culture or cultures. Formed in 2008, the Pacific Nursing Section was the last NZNO section to be established before a moratorium was placed on the formation of new sections in 2011.
The NZNO Constitution was amended last year, through a remit submitted to the NZNO AGM by the Greater Auckland Regional Council, to lift the moratorium and allow the creation of new colleges and sections.
The rationale provided in support of the remit noted that: “NZNO structures need to be flexible enough to respond to the changing reality”. And we’ve seen in the pie charts the changing reality of NZNO membership. The remit rationale added: “Various membership and role classification groups exist without a corresponding NZNO structure to date. Examples include… internationally qualified nurses”.
I will now hand over to Kerri Nuku. Because we will be back as part of the discussion panel after lunch, and because I have used up all of my available time, I would ask that you save any questions until then.
Thank you.
—————–
• See also:‘Too many immigrants’?
