Today I was in Nelson/Whakatū, for the NZNO Top of the South Regional Convention. It was great to be back, with my feet on the Mainland where I come from, on the day before Pink Shirt Day. As you can see, I was dressed for the occasion.
Celebrated annually around the globe, Pink Shirt Day began in Canada in 2007 when two students, David Shepherd and Travis Price, took a stand against homophobic bullying after a new Year 10 student was harassed and threatened for wearing pink. Pink Shirt Day aims to create schools, workplaces and communities where all people feel safe, valued and respected.
My older child Tama is a Year 10 student this year. He’s in the LGBTQI+ club at his high school, and he wears pink. I’m wearing this shirt partly for him. He says it’s ok to tell you this.
But many of us at the NZNO Convention and elsewhere in health, I know, have experienced bullying from people in positions of power.
Perhaps some are facing that situation in our working lives right now.
Bullying takes a terrible toll – not only on us as nurses, midwives and healthcare workers but also indirectly on those we care for, because we can’t give of ourselves fully when we’re anxious, stressed and worried.
In recognition of this, one of the other NZNO Regional Conventions in Palmerston North last month featured a session on bullying, from NZNO Organiser Deb Chappell. It was profoundly insightful and very practical. A few of you may have seen Deb’s presentation at the 2018 NZNO AGM and Conference in Wellington. I first came across it at the Greater Auckland Regional Convention last year.
Some of Deb’s points have stuck in my mind.
Bullies, she said, thrive on secrecy. They work by isolating us from our support networks. They make sure nobody else knows what’s going on. They say to us, we’ll only make it worse for ourselves if we tell.
But as a fellow survivor of bullying, I’m here to tell you that I believe in the message of Pink Shirt Day 2019: “Kōrero Mai, Kōrero Atu, Mauri Tū, Mauri Ora”.
If we speak up and stand together, we can stop the bullying. And as soon as we do that, suddenly the weight starts to lift and it can become so unexpectedly easy.
“DO YOU believe NZNO is a membership-driven organisation, and how confident are you that the voice of the members is being heard?”
This was one of the tough questions put to me by members at the NZNO Central Regional Convention in Palmerston North last month.
It got me thinking. How would we know that NZNO is a membership-driven organisation? What does it look like when the voice of the members is being heard?
Eventually, I decided that when the diverse voices of the membership are being heard, then the priorities of the organisation match members’ priorities. Our dreams and daily frustrations, our heartaches and our innovative solutions become the focus of action by the organisation. NZNO works for us in the same way we work for our patients, residents and tāngata whaiora.
In Palmerston North, I offered only a short answer: “Yes, NZNO is a membership driven organisation to an extent – but it needs to become more so.”
Having thought about it more since, I can now say how to make that happen, because there are four major opportunities this year for members to shape NZNO’s future direction.
Firstly, any member can get involved in their NZNO regional council. Details are under “groups” on the NZNO website.
Secondly, 2019 is an election year for NZNO. In August, members will be able to vote for up to seven directors who will lead NZNO over the next three years. You may even wish to put yourself forward as a candidate, when nominations open in June.
One member, one vote
Thirdly, under the new “one member, one vote” system, all members will have a say – for the first time – on remits. Remits are statements proposing changes to NZNO policy or to our constitution, which outlines such things as the rights and responsibilities of members and who in NZNO has the power to do what.
Voting on these proposals takes place in August, too. The results will be announced at the NZNO annual general meeting (AGM) in September.
Finally, the NZNO board is leading a review of our current five-year strategic plan, which expires next year. Consultation on a new NZNO strategic plan 2020-2025, which will set the organisation’s key priorities and actions for the next five years, happens in late 2019 and early 2020. Once members have given their input, a final draft will be presented for delegates to vote on at next year’s AGM.
If all of this sounds a bit like more work, on top of long hours in paid employment or study – and maybe after caring for family as well – then you’re probably right.
But there’s no easy way round it. Having a greater say means taking more responsibility. If you don’t feel you know enough to cast a vote, for instance, then spend a few minutes finding out. Read the information, talk with your colleagues and work out where you stand.
If you want NZNO to be more membership-driven, then you have to get in the driver’s seat and steer.
When you do, then together we can deliver on the pledge I made on my re-election as president last year, that NZNO will be open and responsive to the members. •
First published in Kai Tiaki Nursing New Zealand, May 2019. Reposted with permission.
At the NZNO Tai Tokerau Regional Convention in Whangarei on 9 May, Kaiwhakahaere Kerri Nuku, Chief Executive Memo Musa and I were invited to be part of a Q&A panel. We were asked ten questions, sourced from NZNO members in the Region and provided to us earlier in the week.
At NZNO Tai Tokerau Regional Convention: (l-r) NZNO President Grant Brookes, Organiser Odette Shaw, Regional Council Chair Sacha Young, Delegate Tammy Von Keisenberg.Martin, a delegate at Whangarei Base Hospital, asks a question at the NZNO Tai Tokerau Regional Convention.
The questions reflected some common concerns which have been aired at all six NZNO Regional Conventions held so far, such as the independent review of the DHB MECA, and some local concerns specific to Te Tai Tokerau. After dividing up the questions between us, I prepared these notes to answer six of them.
1. Can the panel tell us a bit about themselves to assist with introductions? This could include their marital status, children, grandchildren, animals, the region they live in and any hobbies.
Kia ora koutou, thank you for inviting me here today. When I was asked to be part of this panel by your Regional Council, I wrote back and commended them for building member responsiveness and leadership accountability into the convention programme in this way.
When I speak at meetings, I usually introduce myself with a mihi. I see this as part of whakawhanaungatanga, the establishing of connections by way of whakapapa. Answering this question will be a little bit like that, making connections with you by sharing something else about myself.
So to answer the question, I am “happily unmarried” to my partner of 22 years, Linda. Together we have two children, Tama (aged 14) and Rosa (aged 11). At our home we have one cat and one rabbit. Although I’m originally from Ōtepoti/Dunedin, I am now a naturalised Wellingtonian.
2. Can you describe what your role is and how is it different from the others on this panel.
I would like to answer this question in some depth, referring to our core documents.
The framework for my role as President is defined in Clause 17 of the NZNO Constitution, which says:
“The President and Kaiwhakahaere shall be the joint heads of NZNO, whose functions shall be to:
17.2.1 Be spokespeople for NZNO where appropriate;
17.2.2 Act in accordance with the position descriptions laid down by the Board of Directors;
17.2.3 Consult with… the other officers of NZNO in furthering the objectives of, Annual and Special General Meetings and the Board of Directors; and
17.2.4 Attend and preside over all Annual and Special General Meetings and meetings of the Board of Directors.”
Those “other officers of NZNO” I need to consult with are the Kaiwhakahaere, Tumu Whakarae, Vice-President and the Chief Executive Officer. So currently that’s the two people here with me on this panel, plus Titihuia Pakeho and Cheryl Hanham.
The position description which has been laid down by the Board is available on the NZNO website. It describes my role in more detail. For example, it says:
“As joint heads of NZNO the President and the Kaiwhakahaere shall;
Be the public face of the Board of Directors and NZNO membership
Be spokespeople for the NZNO Board of Directors and NZNO members on matters of policy and strategy, speaking with one voice.
Co-chair meetings of the Board of Directors, the Annual General Meeting and any Special General Meetings of NZNO
Serve the legitimate collective interests of all NZNO members
Have oversight of NZNO’s external relationships
Have oversight of NZNO’s membership groups and networks
Support the Board in effective governance.”
Over all, I think the three broad areas in my position description are oversight of the membership, managing relationships with external stakeholders and governance.
My position description also talks about how my role relates to Kerri’s role, as Kaiwhakahaere. It says: “In essence this is a job share situation requiring negotiation between the President and Kaiwhakahaere as to the performance of their shared responsibilities.”
So while Kerri has some additional responsibilities relating to her role as leader of Te Rūnanga, as the joint heads of NZNO our roles are exactly the same. Although we may not look like it, we’re actually interchangeable.
In terms of how my role differs from the Chief Executive, my position description says: “The role of the President is governance leadership. The President has no authority to direct or constrain the chief executive in the authorised and legitimate performance of her or his management duties. NZNO staff do not report to the President.”
So in summary, the President co-chairs the Board, which appoints the Chief Executive. The Chief Executive controls the staff. In the most general terms, the Board determines “what” needs to be done by NZNO; the Chief Executive and his management team decide “how” to do it.
Finally, it’s important to stress the limitations on my role. My position description says: “The President… has no authority independent of the authority of the Board as a whole. The President must… seek approval or confirmation of action taken on behalf of the Board”.
To make the point absolutely clear, it adds: “The President has no authority to unilaterally change any aspect of Board policy”. So in terms of power and authority within NZNO, my role sits underneath the Board of Directors.
That’s the long answer, describing my role and how it compares. I hope it’s helpful.
3. What is NZNO’s position on climate change and how active are we and where is the accountability?
NZNO developed a position statement on climate change in 2016. This was a result of a policy remit which was passed at the NZNO AGM in 2015. The position statement outlines NZNO’s commitments. These include:
“NZNO commits to collaboration with other health professions to lobby for government ratification of enforceable climate change treaties, and to meaningful action to reduce New Zealand’s contribution to global warming, including a substantial reduction in gross domestic emissions, an end to fossil-fuel subsides, and a moratorium on deep sea oil drilling and fracking.”
The big news on action to reduce New Zealand’s contribution to global warming, released yesterday, was the unveiling of the government’s Zero Carbon Bill (ZCB).
In fulfilment of the commitment in our position statement, NZNO participated in the ZCB consultation last year, in collaboration with OraTaiao – the New Zealand Climate & Health Council. Among other things, we called for net zero emissions by 2040, across all greenhouse gases. Unfortunately, the bill contains neither of these goals – and neither are its targets enforceable.
Launching the ZCB yesterday, Prime Minister Jacinda Ardern distinguished between “carbon” and “methane”. We all do some biochemistry as part of our undergraduate nursing education, so everyone here probably knows that methane, which accounts for about half of New Zealand’s emissions, is also a carbon-based molecule, just like carbon dioxide. And tonne for tonne, it has approximately 80 times the Global Warming Potential of CO2 over a 20-year timeframe. So the government’s failure to take meaningful action through the ZCB means that NZNO will need to keep working hard in the select committee stage of the bill.
NZNO also participated in the earlier review of the Emissions Trading Scheme. Although suggesting improvements, we commented that we are “not assured that it is the most effective or equitable tool to either reduce emissions or address climate change”.
Last year we supported the lobbying efforts of Greenpeace, writing a letter to Jacinda Ardern calling for an end to oil and gas exploration, and we have supported actions on the streets including the People’s Climate March and the recent School Strike For Climate.
Also in our position statement:
“Nurses assert our role and responsibility to contribute to the development of national action plans and policies, and to be part of disaster preparedness to mitigate the impact of climate change on health, and to support to calls for humanitarian assistance wherever health is adversely affected by climate change – especially from our Pacific neighbours.”
Here, we walk the talk. In the wake of Cyclone Winston in 2016, NZNO members joined the New Zealand Medical Assistance Team providing surgical services to affected islands. NZNO donated $5,000 and collected an additional $370 to support the Fiji Nurses Association. In 2018, we donated $5,000 to the Tongan Nurses Association assist with recovery after Cyclone Gita.
“We call for well-designed and resourced public transport and safe walking and cycling routes [here, for example] – developments that, in addition to reducing carbon emissions, would also produce significant health gains.
“We agree that healthy public policy on sustainable, energy efficient housing and urban planning which, in addition to reducing emissions, have the potential to reduce the burden of disease and save energy costs in our poorest families [as in our submission on the Healthy Homes Guarantee Bill].”
“Nurses also advocate specifically for the introduction and enactment of public policies related to reversing the widening deprivation and income gap in Aotearoa New Zealand, which is inextricably linked to health inequalities.
“NZNO acknowledges the knowledge, customs and practices of tāngata whenua and indigenous peoples relating to the protection of the environment.
“We commit to informing and enacting strategies to increase the environmental sustainability of health care, and to reduce waste.”
According to Associate Health Minister Julie Anne Genter, “New Zealand’s healthcare sector contributes between 3% and 8% of New Zealand’s total greenhouse gas emissions. Hospitals, for example, use about twice as much total energy per square foot as traditional office space”.
NZNO is active at the local level in initiatives to reduce this carbon footprint – for example at Counties Manukau DHB, which has reduced its emissions by 21 percent since 2012.
“At an organisational level, we commit to undertake steps to reduce and mitigate our contribution to carbon emissions, including stopping investment in fossil fuels.”
In April 2018, the NZNO Board met with Niamh O’Flynn, Executive Director of 350.org, for advice on how we might do this. As a result, the Board is taking steps ourselves, such as moving to paperless Board meetings. We have commissioned an audit of NZNO’s carbon emissions, to identify areas for attention at the organisational level.
This work is sitting with the Chief Executive. But it has already been decided that when our car fleet comes up for replacement next year, we’ll be looking at hybrid vehicles.
Finally, as you may know, NZNO holds money in reserve to protect against unforeseen events. These investments used to include shares in fossil fuel companies. In 2016, NZNO divested from direct investments in fossil fuels, again as a result of the policy remit passed by members at AGM.
Climate change is a problem so big that you could say that no matter what an organisation is doing, it’s not enough. But I have outlined here some of the actions on our key commitments.
4. Is the MECA report being made available to members?
I will give a very brief answer, quoting from an article in the February issue of Kai Tiaki, and then hand over to the Chief Executive. The article is headed, ‘DHB MECA review under way‘, and says:
“The review’s terms of reference, which were signed off by the board, state the CE will provide the final report to the board “and any other person who, in the opinion of the CE, should receive the report”.
NZNO president Grant Brookes said there was wide discretion around the review’s release. “I believe that transparency will help build trust and heal divisions. So I will be supportive of its release to members, once any information relating to individuals has been redacted, mindful however that the final decision rests with the CE”.”
5. Why doesn’t NZNO have a union shop where we sell promotional material and clothing at cost/subsidised to members?
This is a long story, and perhaps one without a very satisfactory ending.
“Creating a rewards programme” was the top proposal in a paper to the Board from the Co-leaders in August 2016, to address issues of volunteer sustainability, member engagement and leadership development. The proposals came out of a meeting of Chairs of Regional Councils, Colleges and Sections and Te Rūnanga held in March 2016. The paper said, “Rewards may include attractive, culturally appropriate NZNO merchandise”.
In response to this paper, the Board decided to engage a consultant to produce a report on how to improve volunteer sustainability.
That report was eventually delivered to the Board in February 2018. The minutes of that Board meeting record: “The project scope referred to a rewards programme, remuneration of volunteers and providing budget lines for members working on specific projects. The President has concerns that none of these has been considered except for facility time and is also concerned that the report does not reflect the Terms of Reference that were provided. Therefore the next budget for 2019/20 would need to take into account the monetary requirements relating to the volunteer sustainability report.”
Production of NZNO merchandise has also been requested by the Membership Committee, over a long period.
The NZNO budget for 2019/20 was approved by the Board in February. However, I am not aware of any definite plans at this stage to produce promotional material and clothing for sale at cost to members.
6. What do you all do to relax and revive?
Thanks for asking! This is a question which was also asked recently by NZNO Nurse Managers NZNO, in an interview for their quarterly newsletter, Te Wheke. I told them that I recharge by getting out into the “great outdoors” with my family.
The theme of Mental Health Awareness Week 2018 really rings true for me – “Let nature in, strengthen your wellbeing – Mā te taiao kia whakapakari tōu oranga!”.
To maintain my sanity, every now and then I have to get away from wi-fi networks and mobile coverage – preferably under canvas, in the bush or up on the mountain.
But that doesn’t happen as often as I would like. So sometimes I also need to blow away the cobwebs by getting my glad rags on and hitting the dancefloors down on Courtney Place.
Notes of a presentation to NZNO Midlands/BOP/Tairāwhiti Regional Convention today, as part of a leadership session alongside NZNO Kaiwhakahaere Kerri Nuku and Chief Executive Memo Musa.
I thank Diane Dixon, Chair of the NZNO Midlands Regional Council, for inviting me to take part in the NZNO Midlands/BOP/Tairāwhiti Regional Convention.
Ko Ranginui kei runga, ko Papatūānuku kei raro, ko ngā tāngata kei waenganui – Tīhei mauri ora!
Ko te kupu tuatahi ka tuku ki te Kaihanga. Koia rā te timatanga me te whakamutunga o ngā mea katoa.
Kei te mihi anō ki ngā maunga, ngā awa me ngā wāhi tapu o tēnei rohe.
E ngā mate, haere, haere, haere. Rātou te hunga mate ki a rātou. Tātou te hunga ora e huihui mai nei, tēnā tātou.
E te tiamana, ko Diane, me ngā mangai-ā-rohe o Te Rūnanga, ko Tracey kōrua ko Anamaria, tēnā koutou. Ngā whakawhetai ki a koutou mō tā koutou pōwhiri. E ngā kaimahi, me ngā kaiārahi nēhi e huihui nei, tēnā koutou.
Ko wai ahau?
Ko Kapukataumahaka te maunga, ko Ōwheo te awa, ko Cornwall te waka. Ko Don rāua ko Helen ōku mātua, ko Tangata Tiriti tōku iwi, ko Grant Brookes tōku ingoa.
Kua maumahara ahau ki tēnei whakataukī i tēnei ata: “He ora te whakapiri, he mate te whakatakariri”.
Ranginui above, Papatūānuku below, and the people in between – behold!
My first word, I sent to the Creator, the beginning and end of all things. I also acknowledge the mountains, rivers and sacred areas of this district.
I greet those who have passed on, and the living gathered here.
To the Regional Council Chair, Diane, and the Rūnanga reps, Tracey and Anamaria, thank you for your invitation.
To the staff and all the nursing leaders gathered here (which is all of you), greetings.
Who am I?
I hail from Dunedin. I grew up at the foot of Mt Cargill and by the Water of Leith. My ancestors arrived in Dunedin on board the ship Cornwall in 1849. The son of Don and Helen, my name is Grant Brookes.
As we gather this morning, I recalled the whakataukī: “He ora te whakapiri, he mate te whakatakariri”. “There is strength in unity, defeat in anger and division”.
So greetings, greetings, greetings to you all.
It’s good to be here in Kirikiroa/Hamilton. This is the fourth Regional Convention for me so far this year.
In the three previous conventions, I’ve been asked to address three different topics – each under the general theme for this year: “Nurses A Voice to Lead – Health For All”.
Today, I’ve been asked to spend ten short minutes giving some personal reflections on our past year. In this annual review, my words will be words drawn from articles and speeches I’ve written before.
From my perspective, one thing has overshadowed all else in the twelve months since we last met – and that’s the bargaining in the DHB Sector, and its aftermath.
When I stood before you at this Regional Convention a year ago, it was at a different venue – the Eagle Ridge Conference Centre, overlooking the beautiful Tauranga Moana. Our momentous #HealthNeedsNursing rallies, held in the month of April 2018, had just come to an end.
Some of you will remember coming together here in Hamilton, outside the Elizabeth Rothwell Building at Waikato DHB. Others, I’m sure, took to the streets last April outside Tauranga Hospital.
There were rallies at Whakatāne Hospital, on the corner of Lake Rd & Kuirau Park in Rotorua, on the lake front in Taupō – even at Thames Hospital.
Some of you were there on Ormond Rd, at the main entrance to Gisborne Hospital.
For my part, I remember leafleting morning commuters at Wellington Railway Station, and demonstrating with my fellow members outside Wellington Hospital in Newtown.
Those rallies, it turned out, were just the beginning.
The effects of nine years of underfunding, which we highlighted and rallied against during 2017, finally compelled us to take unprecedented industrial action.
For just the second time, nurses in New Zealand’s public health system took nationwide industrial action, alongside midwives and health care assistants covered by the DHB MECA.
For me personally, the hours I spent picketing and marching with my fellow NZNO members on 12 July 2018 will stand as the proudest moments of my nursing career.
The MECA bargaining sparked a campaign of extraordinary drive and determination, on the part of NZNO members and staff alike. Together, we achieved momentous things.
At the beginning, as you’ll recall, most members were being offered three pay increases of 2%, over 33 months, and a lump sum of $350 (pro rata).
When we rejected that offer, the lump sum was increased to $1,050.
After the #HealthNeedsNursing rallies in April and the #HearOurVoices marches in May, the third offer was almost twice as big. The lump sum was bumped up to $2,000. Pay rises ranged from 9.3% to 15.9% over 26 months.
An extra $38 million was pledged by the Government to employ 500 more nurses and $10 million allocated for additional expert nursing staff to support implementation of CCDM.
At the end of July, after two more votes to reject, health minister David Clark put his signature to a new Accord, strengthening commitments to make sure there are enough nurses and midwives in our public hospitals to guarantee safety for staff and patients.
The journey was not easy. We didn’t win everything needed to rebuild our public health system. But every single one of these advances was powered by the unity and determination of thousands of NZNO members, who should be enormously proud of themselves.
Then as Summer arrived, there were signs that the long, cold winter for nursing and for the people we care for was coming to an end.
It will take more struggle yet to clear away all the dark clouds over the DHBs – not to mention the deeper chill still lying across the rest of the sector. But the first of the extra nursing and midwifery staff were being appointed. By the end of Summer in March, just over half of the 500 were in place. Rates of new graduate employment through the ACE Nursing scheme hit record highs.
At the same time, however, there are some unresolved problems. As we faced difficult decisions in the MECA bargaining last year, differences emerged between members, and between members and their representatives. At times there were signs of strife, of the “anger and division” which our whakataukī warns about.
From my vantage point, I’m sorry to say, it appears that these divisions haven’t all healed yet.
As many of you will know, we are in the middle of an independent review of last year’s DHB MECA. This is being conducted by former CTU President Ross Wilson. He has sought the views from all sides of the debates. I expect that his final draft report, which is due in June, will bring together these different perspectives, showing the truth in each and our shared path ahead.
At the same time, the DHB MECA campaign set the pattern for a renewal of NZNO as an organisation which is united, open and responsive to members.
Members last year made the big decisions through democratic votes. We were able to vote online for the first time. This saw the greatest member participation in any decisions in NZNO’s history.
Campaign and LPS planning took place through cooperation between NZNO staff and member leaders, from local workplace delegates to the nationally elected board. Actions were designed to maximise member participation.
It’s democracy and participation like this that has the power to forge unity, out of division. A democratic vote can resolve many individual differences into one collective union decision. As we continue the democratic process of overcoming differences, strength will grow; “he ora te whakapiri”.
Looking ahead, there are three major opportunities this year for members to participate in the democratic process and shape NZNO’s evolution.
First up, 2019 is an election year for NZNO. In August, members will be able to vote for up to seven directors who will lead NZNO over the next three years.
Secondly, under the new “one member, one vote” system, all members will have a say – for the first time – on remits. Remits are statements proposing changes to NZNO policy or to our Constitution, which outlines such things as the rights and responsibilities of members and who in NZNO has the power to do what. Voting on these proposed changes takes place in August, too. The results will be announced at the NZNO AGM in September.
Finally, the NZNO Board is leading a review of our current five-year strategic plan, which expires next year. Consultation on a new NZNO Strategic Plan 2020-2025, which will set the organisation’s key priorities and actions for the next five years, happens in late 2019 and early 2020. Once members have given input, a final draft will be presented for delegates to vote on at next year’s NZNO AGM.
But healthy democracy is more than simply majority rule.
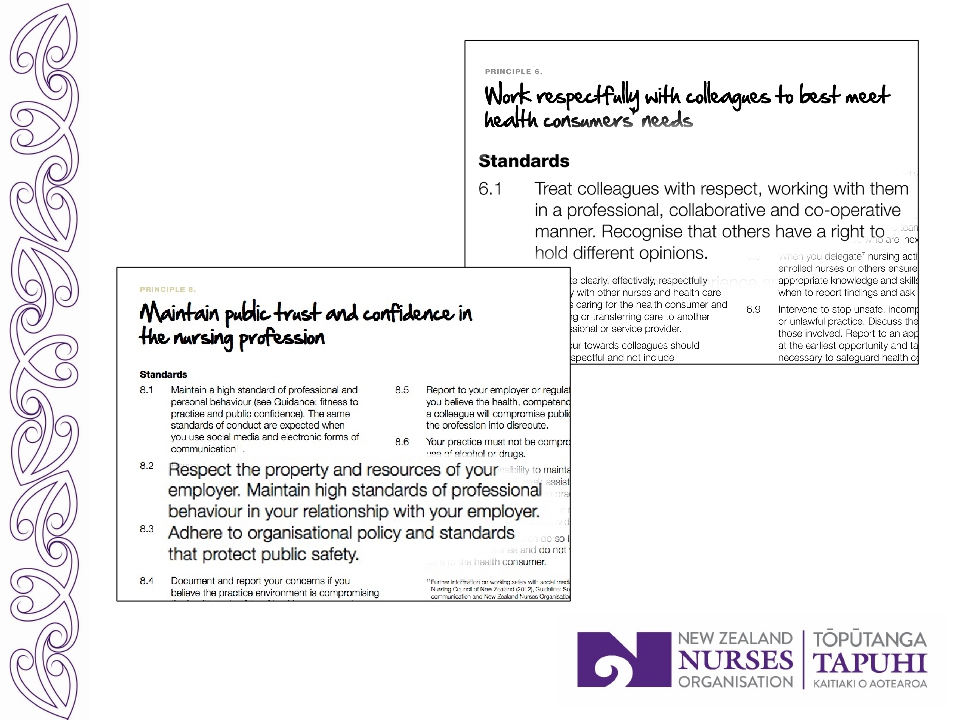
Our professionalism reminds us to work respectfully with colleagues, who may be in the minority. It reminds a majority that others have a right to hold different opinions – and to remain collaborative towards them.
In conclusion, only once before in New Zealand – back in 1989 – have nurses taken nationwide industrial action. That mobilisation reshaped nursing and four years later, in 1993, led to the birth of NZNO.
The winds of change blowing this last year will also be felt beyond the DHBs.
The surge which has drawn unprecedented numbers members into action is bound to power the ongoing transformation of NZNO.
These notes of a presentation to NZNO Greater Wellington Regional Convention on 30 April 2019 were amended on 4 June 2019, to clarify the current position of CCDM implementation at Hutt Valley DHB. I wish to apologise that I did not make this sufficiently clear at the Convention.
Photo courtesy of Shammi Kumar.
E ngā reo, e ngā mana, e ngā karangarangatanga maha o te rohe – tēnā koutou.
Ka tū ahau ki te tautoko i te karakia timatanga. Ka mihi anō ki ngā maunga, ngā awa me ngā wāhi tapu o te mana whenua.
E ngā mate, haere, haere, haere. Rātou te hunga mate ki a rātou. Tātou te hunga ora e huihui mai nei, tēnā tātou.
E te tiamana, ko Rerehau, me te mangai-ā-rohe o Te Rūnanga o Aotearoa NZNO, ko Lizzy, tēnā kōrua. Kei te whakawhetai ahau ki a kōrua mō tā kōrua pōwhiri.
E te rangatira kua hoki mai nō tāwhiti, tēnā koe Kerri. E ngā kaimahi, me ngā kaiārahi nēhi e huihui nei, tēnā koutou.
Ko wai ahau?
Ko Kapukataumahaka te maunga. Ko Ōwheo te awa. Ko Cornwall te waka. Nō Ōtepoti ahau, engari kei te noho ināianei ki Pōneke. Ko Don rāua ko Helen ōku mātua. Ko Tangata Tiriti tōku iwi. Ko Grant Brookes tōku ingoa.
Ka maumahara ahau ki tēnei whakataukī i tēnei wā: “Te Amorangi ki mua, te hapai o ki muri”.
To the authorities, the voices, all the many alliances and affiliations of this region, greetings.
I stand to support the greetings to the Creator, to whom belong all things. I also acknowledge the mountains, rivers and sacred areas of the indigenous people with authority over this place.
I greet those who have passed on, and the living gathered here.
To the Chair, Rerehau, and the Rūnanga rep, Lizzy, thank you for your invitation.
To the chief returned from afar, greetings to you Kerri. For those who may be unaware, Kerri is just back from New York where she addressed the UN Permanent Forum on Indigenous Issues and is due to arrive at this Convention very soon.
To the staff and all the nursing leaders gathered here (which is all of you), greetings.
Who am I?
Although I now live in Wellington, I hail originally from Dunedin. I grew up at the foot of Mt Cargill and by the Water of Leith.
My ancestors arrived in Dunedin on board the ship Cornwall in 1849. The son of Don and Helen, my name is Grant Brookes.
For reasons I will soon explain, at this time I recall the saying: “The leader at the front and the workers behind the scenes”.
So greetings, greetings, greetings to you all.
So many old familiar faces. It’s wonderful to be back here with you again.
——
The theme of today’s convention is the one set by the International Council of Nurses (ICN) for the upcoming International Nurses Day on the twelfth of May. “Nurses: A voice to lead – Health for all”.
In keeping with this theme, the topic I’ve been asked to speak on is the following (it’s a long one!):
“Nurses, HCAs and Midwives face a number of issues on the shop floor on a daily basis, while working for the health of New Zealand… we ask that you speak with the aim of motivating and inspiring our members to harness/channel their momentum, energy and input into health for us as members.
In doing so, please include information on anticipated changes off the back of the MECA, a summary of the current campaigns, how the various health sectors can communicate with and support each other with these campaigns, and any plans around the organiser structure to support this.”
It was this suggested topic that made me think of the whakataukī, “Te Amorangi ki mua, te hapai o ki muri”. Literally, “The leader at the front and the workers behind the scenes”, this saying expresses the general idea that everyone is of equal importance.
Or as former Minister of Māori Affairs Te Ururoa Flavell has explained, the late Wiremu Tawhai “provides a far richer meaning [for this whakataukī] which is expressed in terms of sustainability and survival. He suggests the mana of the whole group is dependent on the support and guidance provided by ‘te hapai o’.”
It occurs to me that the same is true for health and wellbeing. The health of the whole group is dependent on the health of those who do the work of delivering healthcare. So when we talk about “health for all”, we must consider health for us.
“All over the world, there are individuals and communities who are suffering from illness due to a lack of accessible and affordable health care. But we must also remember that the right to health applies to nurses as well! We know that improved quality and safety for patients depends on positive working environments for staff. That means the right to a safe working environment, adequate remuneration, and access to resources, and education. We must add to this the right to be heard and have a voice in decision making and policy development implementation!”
I have opted today to talk in detail about a handful of key developments, rather than offer a broad brush overview. If you miss any of the facts and figures in my talk and want to find them later, my speech notes will be available on my blog at nznogrant.org.
So firstly, what can we anticipate off the back of the DHB MECA?
‘Immediate relief’?
When the collective agreement was ratified in August last year, it came with $38 million in extra funding from the Ministry of Health for “immediate relief on staffing and workloads” and a promise of “500 extra nurses”. Without this movement on positive working environments in DHBs, this access to resources, then improved quality and safety for patients will be very hard to achieve.
Eight months on, where are we at?
According to the latest update issued by the Ministry of Health, as at 13 March, 222 FTE registered and enrolled nurses, 19 FTE midwives and 42 FTE Health Care Assistants have been employed as a result of the additional $38 million.
“A further 118.04 FTE are… in recruitment processes… Some DHBs have recruited all their allocated FTE, others have recruited most of it and some have asked to defer a portion of their funding to the 2019/20 financial year.”
So about half the extra nurses promised “immediately” have been employed, with job ads out for a further quarter. Although all DHBs got their share of the extra funding last year, some of them don’t want to (or can’t) spend it all on employing extra staff – or at least, not this year.
In summary, off the back of the DHB MECA we can anticipate what I predicted in Kai Tiaki last December: “It will take more struggle to clear away all the dark clouds over our public health system – and the deeper chill still lying across the rest of the sector”.
To get what we’ve been promised by employers, we’re going to have to hold their feet to the fire. This struggle will require a whole-of-organisation effort. But crucially, the struggle will now take place under conditions which are more favourable than before the DHB MECA settlement.
This is a theme that will run through the remainder of my talk.
Safe Staffing Accord
Also off the back of the DHB MECA, of course, was the Safe Staffing Accord between the Ministry of Health, NZNO and the DHBs. The Accord contains three commitments. The first of these is the one where we may anticipate the biggest and fastest progress. It says the parties will “explore options for providing employment for all nursing and midwifery graduates…”
The latest available report on the Advanced Choice of Employment Nursing intake, dated November 2018, shows that 85.7 percent of the 468 mid-year applicants received a place in the Nurse Entry to Practice (NETP) or Nurse Entry to Specialist Practice (NESP) programmes.
This compares with a new grad employment rate of 54.6 percent in 2016 and 64.8 percent in 2015.
Preliminary data for the 2018 end-of-year intake show that as of January 2019, 71.3 percent of the 1,253 applicants had been placed. This number will rise when the final report is released in July.
CCDM
The second commitment in the Safe Staffing Accord links directly to the Terms of Settlement for the DHB MECA – to “develop any accountability mechanisms the Parties believe are necessary (over and above those already agreed) to ensure DHBs implement the additional staffing needs identified by CCDM within the agreed timeframe” of 30 June 2021.
Hand on heart, I cannot say I expect all DHBs to achieve this, if left to their own devices. I base this on some information which I’m not at liberty to share but also on past experience, which will be very well known to some of you here today.
Hutt Valley DHB commenced implementation of CCDM back in 2013. In March 2014, Board meeting minutes record that “The Coronary Care Unit was selected as the Pilot Ward for Part 1 of the CCDM Programme… There was excellent buy-in to and engagement with this from all staff; nurses, doctors, allied health, clerical and health care assistant staff. The data is still being entered and then will be analysed.”
By January 2015, staffing methodology (which at that time was called the “Part 2 mix and match calculation”) had been completed for three inpatient areas, setting their base nursing FTE requirements, and was under way in a fourth ward as well.
But then, after changes in the Executive Leadership Team during 2015, a full external review of CCDM was commissioned by the DHB (see this link). The FTE calculations, which had showed that extra nursing staff were needed, got shelved.
“Recalling this history is not to make any comment about HVDHB now. HVDHB is in fact well on track to have CCDM fully implemented by June 2021, with support from across the DHB and Board and an excellent relationship with NZNO and the Safe Staffing Healthy Workplaces Unit. Rather, it is to remind us what to look out for elsewhere, and what we need to do to help make sure all DHBs follow through on their CCDM commitments.”
So I anticipate that winning increases in baseline staffing off the back of the MECA is another change that will require a whole-of-organisation effort – from nurses on the floor entering their Trendcare data, to delegates pressing for oversight through local data councils for their ward. Delegates must blow the whistle, for instance, on any manager who alters Trendcare data after it’s been actualised. And they must have paid release time to do this and other CCDM work.
Organisers, Professional Nurse Advisors and senior delegates on the DHB’s CCDM council must demand adherence to the programme and to timelines. FTE calculations must be accurate and acted upon, even if it means cost increases. And people like me and Hilary Graham-Smith must ensure DHB accountability through the Safe Staffing Unit Governance Group, while Chief Executive Memo Musa does the same there and in the Health Sector Relationship Agreement Steering Group and the Safe Staffing Accord Operational Group.
The pace and scale of implementation means I expect workloads to increase over the next two years. But again, we’ll be working under conditions more favourable than before. At last, there is a deadline for CCDM implementation. The Minister of Health himself has requested regular progress reports.
Pay equity
The final development off the back of the DHB MECA which I’ll discuss is pay equity.
NZNO raised a pay equity claim as part of the MECA negotiations. DHBs acknowledged that nursing has been undervalued. A pay equity process with an implementation date of 31 December 2019 was agreed.
Soon, expressions of interest will be sought from NZNO delegates at the DHBs chosen to participate in the assessment process.
After that, claimant (our) data will be gathered through interviews with job holders, including senior nurses, registered nurses, public health nurses, nurse practitioners, enrolled nurses karitane nurses, obstetric nurses and health care assistants including psychiatric assistants. This part of the process will take through to late September/October. The pay equity claim for NZNO’s midwifery members will be progressed in a concurrent but separate process. The interviews will be conducted using pay equity assessment tools that have been purposefully developed to be gender-neutral.
Finally, an NZNO bargaining team will be democratically selected. The union team will use the assessment data and comparisons to negotiate and conclude a pay equity claim. Ratification will happen when an agreed outcome has been identified based on the evidence, between the DHBs and union negotiating team. I expect this work will occur between early November and late December.
At this stage I anticipate that the deadline will be met, but I am also aware that the timeframe for completing the work in time for implementation by 31 December is very tight.
In Safe Hands
Regarding current campaigns, and how the various health sectors can support each other, last month saw the launch of what will be NZNO’s flagship campaign for 2019. “In Safe Hands” is calling on the government to review and update the Aged Care Safe Staffing Standards, to set minimum staffing levels based on residents’ needs.
Stage one of the campaign seeks to sign up NZNO members from all health sectors as activists and asks them to send an initial message to the Government. You can get involved at www.insafehands.co.nz.
Without this campaign, I would expect that trends of reducing care hours and increasing workloads – identified in new research from Dr Julie Douglas and Associate Professor Katherine Ravenswood of AUT – are likely to continue across the aged care sector.
Based partly on initial reactions when we raised it with the Minister of Health, I anticipate that achieving the goal of this campaign is going to be hard. But together, with the whole organisation behind us, we can do it.
PHC MECA
The Primary Health Care Sector is another where we will have to struggle to achieve the ambitious goals around positive working environments, adequate remuneration and health for us as members, within very tight timeframes.
The Terms of Settlement for the PHC MECA, which was ratified last month, contained an agreement that employers and NZNO will undertake a joint exercise to scope the nature of Health Care Assistant, Nurse Practitioner and Designated RN Prescriber roles within PHC by 31 August 2019. That’s just four months away.
It also said: “NZNO and NZMA have agreed to jointly lobby government as soon as is possible and no later than April 2019 to increase funding to the sector to enable the sector to be able to recruit and retain nurses and to meet expectations regarding nursing salaries following the DHB settlement”.
In particular, increased funding will be essential to securing new steps 6 and 7 in the next PHC MECA negotiations, as in the DHB MECA, and any pay equity process that might be agreed in future. I probably needn’t remind you that today is the 30th of April 2019.
Also within the PHC Sector are Māori and Iwi providers. Here I am optimistic enough to finally predict – after more than a decade of work led by Kerri and Te Rūnanga – movement this year on the issues of inequitable funding models and pay disparities.
Violence in the workplace
A second campaign will address one of the six Global Health Challenges highlighted in the ICN Guidance Pack for International Nurses Day: “the effects of violence on health care and all of us”.
“Violence is an everyday occurrence around the world for health workers”, says ICN. “This includes violent physical, sexual and verbal assault from patients and potentially their families. The issue is so bad that across the world, nursing is considered more dangerous than being a police officer or a prison guard…
“Violence against nurses threatens the delivery of effective care and it violates their human rights. It damages their personal dignity and integrity. It is an assault on the health system itself.”
Health for us as members means freedom from violence at work. To this end, NZNO is producing a “Position statement: Violence and aggression towards nurses”. This will serve as the basis for a campaign. A project team has been established, with leaders drawn from across our organisation.
Before I finish, I was also asked to speak about any plans around the organiser structure to support these efforts and campaigns. I take this to mean the structure of the organising work performed and supported by by NZNO staff.
The annual, weekly and daily planning of this work is an operational matter, under the direction of NZNO management. But I can report on some discussions around resourcing and strategic planning at the Board level.
First of all, earlier this month the Board of Directors approved business cases to increase the number of NZNO organisers by 2.0 FTE during the current financial year. What does this number mean?
This represents a 6% increase in the existing organiser workforce of 35.95 FTE. The last increase in the number of organisers was in 2017, when an extra 1.5 FTE was approved. The increase before that was back in 2007. That year, total NZNO membership sat at 39,000. It is now 52,000. A planned review of organiser resource in 2011 was deferred in favour of setting up the Member Support Centre.
So in the last 12 years, we have seen the establishment of MSC, while the number of members has grown by 33 percent and the number of organisers has been boosted by 10 percent.
To address this mismatch, and current workload issues such as those arising from rapid nationwide implementation of CCDM (noted previously), the initial business case put to the Board in February this year sought an extra 5.0 FTE for the organiser workforce, plus 1.0 FTE for casual or “relief” organising.
The Board decision to approve a lower number than six full-time equivalents was based on the need for a break even operating budget. But clearly, there are issues with sustainability and pressures are building. These pressures could be resolved in a number of ways.
Firstly, business cases declined this year could be funded in the future. Alternatively, the pressures could also be addressed by reorganising the way we work. On a part of the NZNO website you may not have visited, it says:
“Wherever possible, we use the “organising” model which simplistically means, an approach to working with members that empowers them to act in their own interest, with NZNO’s elected leadership and staff on a team basis. This approach is distinctly different from that where a staff or elected member “fixes” things for members.”
“Wherever possible” depends on factors like the number of delegates in a workplace and their skills, confidence, engagement and their resourcing, including the amount of their paid release time, along with the nature of member issues. It also depends on how staff work to empower and educate members.
Clearly, addressing growing pressures on our organiser structure is not a case of “either/or”. A combination of more staff and changing the way we work is possible.
This concludes my talk. Thank you for listening. I will be available to answer any questions now and throughout the day.
“Te Wheke” is the quarterly newsletter of NZNO Nurse Managers NZ, the professional section of NZNO dedicated to sound nursing management and leadership. I was humbled to receive the offer of an interview for the regular “Spotlight Interrogation” feature in the March 2019 issue – now hot off the press, and re-posted here with permission. Thanks to editor Shamim Chagani for this opportunity to get “up close ‘n’ personal” with readers.
Spotlight interrogation
1. What’s your name, what do you do and where do you work?
Kia ora, koutou. Ko Grant Brookes tōku ingoa.
I’m Grant Brookes, President of the New
Zealand Nurses Organisation Tōpūtanga Tapuhi Kaitiaki o Aotearoa.
I work out of the NZNO National Office in Wellington, but I also travel around to engage with as many members as possible. Being accessible is important to me. I welcome contact by phone (027 536 2851), email (grant.brookes@nzno.org.nz) or via your preferred social media platform.
2. What would you be doing if you were not working at your current job?
If I had not been elected NZNO President in
2015, I would be working as a Staff Nurse at Wellington Hospital.
It’s a job I love. I still miss the patient contact, the collegial relationships in the multi-disciplinary team and the hands-on care. I continue to work the occasional shift on the ward, to keep my feet on the ground and my clinical skills fresh. I may even go back to it when my term as President ends in 2021.
3. What’s the most important lesson you’ve learned in the last year?
This last year has reaffirmed an old truth,
and taught me something new.
For me, 2018 proved once more that solidarity is powerful. By standing together with one another, and with our communities, NZNO members in the DHBs may not have fully restored our health system. But through our rallies, marches, votes and strikes, we did secure an extra $250 million in health funding, on top of what the DHBs initially offered, and an immediate 2% increase in nursing FTE. As the old union song proclaims, “Solidarity forever, for the union makes us strong”.
I’ve also learned a new lesson. As a Pākehā male, I’ve been aware all my adult life that even as a working class kid from South Dunedin, I was born with a degree of privilege. I long ago vowed to use that not for my own benefit but to raise up those without, so that unearned privilege might one day cease to exist. It’s probably why I went into mental health.
But 2018 taught me, perhaps belatedly, that when working within power structures we must also advocate for ourselves. I was recently struck by one of those Facebook shareables. It said, “Be careful what you tolerate, you are teaching people how to treat you”.
4. What characteristics do you most admire in others?
The characteristics I admire most in others
include emotional intelligence, analytical power, commitment to a win-win
outcome and above all, integrity.
I think the world needs more people like that.
5. What qualities in you would you hate to see emulated in your employee?
As NZNO President my role is governance, rather than management. I have never been in a position where I employed someone. But if I did have employees one day, I would certainly hope they were better at striking a work-life balance than me!
6. If you were to start a company from scratch, what values would you build it on?
If I was to build a company from scratch, it would probably be a cooperative. It would be founded on values of shared ownership, teamwork and public good.
7. If you were to tell one person “thank you” for helping me become the person I am today, who would it be and what did they do?
There have been so many people who have
helped me to become the person I am, I could never thank just one.
I have spoken before, in Nursing Review, about the formative influence of my mother.
But I would also thank my activist colleagues from the student protest movement of the 1990s (some of whom are now also leading unions, advising government ministers, or in one case – Grant Robertson – being a minister themselves!).
I would thank my mentors from the new graduate programme at ADHB, without whom I would never have stayed in the profession, and my NZNO organisers at Capital & Coast DHB. The best single piece of advice I ever received came from them. Having been rapidly elevated as young NZNO delegate onto a CCDHB clinical governance committee, and having struggled in meetings with “imposter syndrome”, my organiser looked me in the eye and said, “take your seat at the table like you were born to be there”. It worked.
I would thank my partner of 22 years,
Linda, who taught this white kid to love reggae, and our children, Tama and
Rosa, who made me a dad.
I would thank Joyce and Roimata, two of the
many unacknowledged giants now holding up the Māori Women’s Welfare League, who
shared with me so generously of their matauranga Māori through our years of
work together.
I wish I could thank Helen Kelly, for her quiet,
consistent encouragement.
And finally I would thank NZNO CEO Memo Musa and Kaiwhakahaere Kerri Nuku, who have both taught me more about leadership in the last three years than they will probably ever realise.
8. When are you happiest?
That’s easy – and probably easily relatable for any other powder hound. I’m happiest when I am on the slopes.
9. What one memory do you most treasure?
Does it say something about my age and
stage that my treasured memories are now of my children? Those memories are all
full of “firsts” – first steps, first words, first day at school, and on and
on.
I remember them all. The days our two were born, at home, are probably the most treasured memories of all.
10. What would a “perfect day” look like for you?
A perfect day for me is when I get a win for my fellow NZNO members.
11. How do you recharge?
I recharge by getting out into the “great outdoors” with my partner Linda and our kids, Tama (aged 14) and Rosa (11).
The theme of Mental Health Awareness Week
2018 really rings true for me – “Let nature in, strengthen your wellbeing – Mā
te taiao kia whakapakari tōu oranga!”.
To maintain my sanity, every now and then I have to get away from the city and from screens with them – preferably under canvas, in the bush or up on the mountain.
12. What superpower would you like to have?
In January our sister union in the US, National Nurses United, posted this meme on their Facebook page ahead of the 2019 global #WomensMarch. It features my friend and colleague, NNU Co-President Deborah Burger (front row, second from right). This meme about sums it up for me.
At the NZNO Central Regional Convention in Palmerston North on 9 April, Kaiwhakahaere Kerri Nuku, Chief Executive Memo Musa and I were invited to be part of a Q&A panel. We answered eight questions, sourced from NZNO members in the Region and provided to us the week before.
Three of the questions were addressed to me. Here are the notes I prepared, for use in my answers.
Question 1. Social media is a growing factor in communication and in influencing opinion. What is NZNO’s strategy and safeguards in relation to social media platforms?
Firstly, thank you for the opportunity to participate in your Regional Convention in this way. When I received the invitation to be part of this panel from your Chairperson, Trisha Hurley, I wrote back and commended the Central Regional Council for building member responsiveness and leadership accountability into today’s programme.
Turning now to the question, I would like to clarify what we mean when we talk about NZNO. What might pop into your head when you hear “NZNO” are the staff who work in our NZNO offices. But I’m really clear in my mind that “NZNO” means the 52,000 of us who are part of this organisation, each with with our own role to play in successfully delivering NZNO’s strategies.
Social media is a topic I spoke on at the Southern Regional Convention in Dunedin, the week before last. The notes from that presentation are available on my blog.
In my speech the week before last, I also mentioned the upcoming CTU Organising Conference, held in Auckland last week.
As anticipated, social media strategy was a major theme running through the conference. It featured in the three keynote speeches from international guests. Carl Roper from the UK spoke about the work of the Trades Union Congress Digital Lab, which supports research, leadership and training in digital transformation. Melanie Gatt & Felicity Sowerbutts from Australia showcased recent successful social media strategies in Sydney and Melbourne.
Much of the learning at the conference was focused on digital unionism, although NZEI Te Riu Roa (which is both a union and professional association, like us) presented on their new social media strategy for teachers in Early Childhood Education. And a values-based communication workshop run by the Post Primary Teachers Association Te Wehengarua – also a professional association – covered social media campaigns.
A number of key points for came through all of this. Firstly, and most obviously, was the need for a strategy. The point was made repeatedly that if we don’t lead the debates about our issues on social media, then other people will.
Secondly was the importance of using Facebook groups – either by joining large existing ones (like the 35,000-strong “NZ teachers” group), or by setting up new ones (like the “PPTA members – bringing out the best” group, created by the comms team at the secondary teachers union).
Thirdly, it is essential to interact. The power of social media lies in its interactivity. Using social media like a noticeboard, simply posting messages and then walking away, won’t work. In fact, it may be worse than doing nothing.
Fourthly, this social media interaction must be member-led. This is not only a practical necessity, given the 24/7 nature of interaction on these platforms, it’s also key to maintaining credibility. But equally, our volunteer digital activists need support from union staff, including training and mentoring. Private Messenger groups bringing together communications staff and member activists was highlighted as a good way to provide support, allowing debriefing and problem-solving in what can be a very challenging environment.
If those were some of the learnings from the CTU conference, what then is NZNO’s strategy?
The short answer is that unfortunately, we don’t yet have an overall strategy. A framework for developing an NZNO social media strategy does exist. It came out of a communications review commissioned by the Board and completed in 2017. But implementation of the review recommendations has been delayed, partly due to resource constraints.
In the absence of an overall strategy, what we have at present are discrete social media campaigns, a range of practices by different actors within the “NZNO 52,000”, a range of views on how to approach social media, and a few decisions and actions regarding social media. These decisions tend to be reactive and ad-hoc.
I will conclude by giving some examples from Board level. There, some decisions and a range of views are documented in the Board meeting minutes, which are available to members on the NZNO website.
The minutes of the meeting held on 15 February 2017, for instance, record that: “The Board expressed concern that the President is still reporting personal blogs [and other social media activity] toward his key performance indicators (KPIs) which is not part of Presidential work. The President responded that the work plan approved by the Board contains reference to [social media] KPIs and these are what is being reported on, and that he sees this as part of member engagement.”
So there you can see clearly that there was a range of views, in this instance over whether member engagement on social media should be part of my work as President.
“Regarding social media”, the minutes continue, “a Board member has observed that there is an “NZNO” Facebook group which is not an official one. The communications review may inform the use of the unofficial and official Facebook pages. A board member commented that on more than one occasion use of the unofficial Facebook group has caused problems. A request is to be put in writing to the administrators of the unofficial Facebook group containing recommendations to remove the NZNO branding…
The Vice President is to draft a letter to the administrators of the unofficial Facebook group to request removal of NZNO branding. The letter, once approved, is to be sent on behalf of the Board to ensure the message is clearly received that this was a decision made by the Board.”
This decision reflects one approach to social media strategy, agreed by the Board.
Incidentally, I had been an administrator of that unofficial “NZNO Members and Supporters” Facebook group at that time, supporting the team of NZNO delegates who moderated and led the debates, and part of their private Messenger group. After the meeting, I was obliged to give up that admin role.
Decisions on social media activity were also made at the following Board meeting, on 19 April 2017.
The minutes record: “The Board observed that who makes the posts plays an important part in social media. NZNO’s Employment Lawyer has advised that while NZNO may look to ensure that the right of freedom of expression does not override any specific legal duties and obligations by way of its formal moderation for official NZNO Facebook posts, it is not clear as to how much (if any) oversight might be extended to unofficial Facebook posts in the absence of formal NZNO moderation of same.
The Board discussed the President writing a second article for Kai Tiaki as a way to inform members. The Board instructed the CE to request that Kai Tiaki journalists write a brief article covering the Employment Lawyer’s opinion for the next issue of Kai Tiaki.”
Again, on 15 August 2018, the Board minutes record: “A member of the Negotiating Team believes there needs to be moderation of sites with NZNO’s name attached. The President advised that he had looked in February and at that time there were 41 unofficial websites Facebook sites with NZNO’s name attached”.
A resolution was passed: “That a letter from the Board be sent to unofficial NZNO Facebook site administrators requesting that they cease to use abbreviations NZNO and associated NZNO branding on the unofficial Facebook sites they administer.”
This resolution has not yet been implemented.
Question 2. Do you believe NZNO is a membership driven organisation and how confident are you that the voice of the members is being heard? How valuable are Regional Councils in the NZNO structure and do they serve their intended purpose?
This is a two-part question. If it’s ok with you all, I will deal with the first part quickly.
Do I believe NZNO is a membership driven organisation and is the voice of the members being heard? Yes, to an extent, but it needs to become more so.
The second part is about Regional Councils. I’d like to take some time to look at why we have Regional Councils. What are they? Where do they come from? What is their purpose? Do they make the voice of members heard?
Regional Councils are one of the five fundamental membership structures mandated by the NZNO Constitution. The other four structures are the workplace delegates, colleges and sections, the National Student Unit and a little-known body called Health Professionals NZ. You can find out more about these in Schedule Seven of the Constitution, on the NZNO website.
The origin of Regional Councils is described on pages 209-10 of NZNO’s official centennial history, “Freed to Care, Proud to Nurse” by Mary Ellen O’Connor:
“By 1988, there were 54 branches of [the New Zealand Nurses Association]… In 1989 a major restructuring took place. Branches, which facilitated remits and conference voting, were abolished in favour of… individual membership of NZNA, with workplace groups being the first point of reference and the eleven regional councils being the next. All these regions would have representation on the new NZNA national council, bigger than the old national executive…
“This restructuring was seen by NZNA leadership as better representing the majority of members, who now worked across multiple workplaces. It was perceived by the membership, however, as the destruction of the organic channels that they had created.
“In fact, the imposed structure was never to function in the comfortable, rhythmic way that the old branches had.”
So there you have it. In the opinion of the author of our official history, compared to the previous structures Regional Councils have never functioned to make the voice of members heard.
This excerpt from our history also talks about some of the other purposes of regional councils.
Each regional council decided on their “representation on the national council”, the governing body known today as the Board of Directors. That purpose was removed in 2012, when election of directors was transferred to an all-member ballot.
And the regional councils “facilitated remits and conference voting”. Conference voting has also been removed, now replaced by the “one person, one vote” system.
The remaining purposes of these structures are set out in the NZNO Regional Council Handbook. This document is currently under review. The new version will be out very soon. The current version is seven years old, and still refers to the functions now removed, but where it’s not outdated it says:
“In general, Regional Councils are critical for the information flow and promulgation of NZNO policy between the Board of Directors and general membership within the region. They also play an active role in the successful operation of Regional Conventions [and congratulations to Trisha and your council for organising today’s great event], management of any regional funds… management of consultation documents and submissions, regional activities such as International Nurses Day, projects and the operation of any sub-committees.”
Do Regional Councils serve these purposes? Given that they are heavily dependent on the precious time and effort of our wonderful volunteers, I think that by and large they do these things as well as they can.
But the questions remain. Is this what they were intended to do when they were created? And are they the best structure for ensuring that the voice of members is heard?
Because Regional Councils are part of the interlocking, fundamental membership structures in Schedule Seven, if anyone ever decided they needed to change, it would probably require a full review of the Constitution.
Question 3. Members have raised concerns about the amount of overseas travel undertaken by the leadership. Is the overseas travel justified and what benefits does it bring to the average member?
My answer to this question will be in two parts. The first part is about something which can be measured precisely. The second thing is impossible to quantify.
I have a handout to go with my answer. Here is an extract from a paper presented to the NZNO Board meeting on 12 February 2019 by David Woltman, our Manager, Corporate Services.
David prepared the paper at the request of our Audit and Risk Committee, who had heard the member concerns about the amount of overseas travel undertaken by the leadership and responded.
The figures in the table cover travel costs for all NZNO members and staff. As you can see, while costs go up and down from year to year, in 2018 the total gross amount spent on all international travel was $28,163, or roughly 0.1% of the NZNO budget. Twenty times that amount was spent on domestic airfares, supporting NZNO members to attend events like the AGM and Conference, college and section committee meetings, and so on.
I think many would be surprised to see what a small amount goes on international travel. Some of the $28,163 gross spend was later recovered, by the way, through payments to NZNO from sponsoring organisations and individuals.
In terms of the benefit to members from this travel, this is something that’s impossible to quantify, so I won’t even start.
But I would like to read a couple of messages.
“I am writing to you today on behalf of the International Council of Nurses (ICN) following the brutal and horrific attack on two mosques in Christchurch in which dozens of people were killed during Friday prayers.
“We offer our unconditional support to the New Zealand Nursing Organisation, Nurses and all healthcare workers in Christchurch and across New Zealand. The thoughts of Nurses from around the world will be with you, the victims and families of these attacks and we stand resolutely beside you in condemning all forms of violence, harassment, intimidation and discrimination against immigrants and minorities and indeed people anywhere.
“We are deeply saddened by this barbaric act, which goes against all human values and took the lives of innocent people while they were praying. We understand from news reports that 49 people have been killed and more injured including young children with gunshot wounds and that Christchurch hospital was a safe haven during the attack. We acknowledge both the compassion and bravery of the nurses, first responders and all the healthcare staff who provided care immediately after the incident and continue to do so during a time of great pain and grief. Nurses will always provide care for patients whenever and wherever it is needed.
“Our sincerest sympathy and complete solidarity is with NZNO and all the people of New Zealand at this time.
Yours sincerely,
Annette Kennedy, President & Howard Catton, Chief Executive Officer”
This letter was circulated. Its compassion is born of NZNO’s close connections to ICN. I think that members who read it in the days and weeks after the attack, felt better. And for me, that’s the benefit.
One more:
“Nurse leaders around the world joined together in expressing shock and horror at the deadly slaughter in Christchurch, New Zealand and said it is a reminder of the deadly consequences of hate speech, Islamophobia and anti-immigrant policies that must be confronted and challenged by all.
“Global Nurses United, representing nurses and health care workers unions in 23 nations, said they stood in unity with the Muslim community targeted by the attack, and expressed support for New Zealand nurses, represented by the GNU affiliate, the New Zealand Nurses Organisation (NZNO), and other health care workers who are providing care for the victims and their families.
“No nation can be considered democratic when people must live in fear of violence because of their religion, ethnicity, immigration status, or race, said GNU. In addition to the loss of life and injury, there are also long-term consequences that can erode the mental and physical health of affected family members and entire communities and nations for years.
“New Zealand reminds us that this has become a global crisis and must be confronted as a global community.
“It is incumbent on our world leaders to join together in not only condemning the violence, but in directly challenging the inflammatory rhetoric and policies that encourage them.”
I think this sums up why we engage internationally: “New Zealand reminds us that this has become a global crisis and must be confronted as a global community.”
The hate that caused so much grief to so many people – not least, to NZNO members at Christchurch Hospital – is international, and can only be confronted by us connecting internationally.
And it’s not just in moments of tragedy. Global interconnections – involving governments, health authorities, health employers, nursing regulators, educators, nursing policy-makers and researchers and even our families – shape the lives of NZNO members, every minute of every day. This is why NZNO must be there on your behalf, too.
Speech notes of a presentation to NZNO Southern Regional Convention at the Otago Golf Club, Balmacewan, Dunedin, 28 March 2018.
Tihei mauri ora! Te mea tuatahi, ka tū ahau ki te tautoko i ngā mihi ki te kaihanga. Firstly I stand to support the acknowledgement of the creator.
Kei te mihi hoki ahau ki ngā uri whakaheke nā Tahu-pōtiki, te tino tipuna, me ō rātou wāhi tapu katoa. I also acknowledge the descendants of Tahu-pōtiki, the great ancestor of Ngai Tahu, and all their sacred places.
Nō reira, e ngā mana e ngā reo, e ngā karangaranga maha, tēnā koutou. So to all the authorities, all voices and the many affiliations, greetings.
As I speak at meetings around the country, I often talk about my connections to this place. It was here, in Ōtepoti/Dunedin, that my ancestors arrived from Scotland back in 1849, aboard the Cornwall.
Behind me I know that Mount Cargill, Kapukataumahaka, is looking down on us, as it always has. Out there beyond the trees, I see my old high school, where I returned last year for the school centenary. And over the ridge line, I know that Ōwheo, the water of Leith, winds its way to the sea.
It’s wonderful to be back home, on my tūrangawaewae, the home where my feet belong.
The topic I’ve been asked to speak on today is, “The impact of social media on NZNO members, delegates and on NZNO’s reputation”. It’s a sensitive topic. It is also very large.
My talk will not be a definitive, or comprehensive account of the impact of social media.
As you may be aware, a review of the DHB MECA bargaining process and supporting campaigns is currently being conducted by former CTU President Ross Wilson. The terms of reference for the review direct him to “Enquire into and comment on NZNO’s… processes for communications (internal and external) including the use of social media”. We keenly await his findings, which are due to be delivered to the NZNO Board in June. After that, we will be in a better position to evaluate thoroughly the impact of social media on NZNO members, delegates and on NZNO’s reputation.
Even this time next week, I would be better placed. At the CTU Organising Conference in Auckland on Wednesday, there will be an NZNO presentation on, “Lessons learned from the major state sector industrial campaigns of 2018”. No doubt this will cover the impact of social media, as well.
So what are we talking about, when we speak of social media?
Social media is defined in our Guideline as the “internet or web-based technologies that allow people to connect, communicate and interact in real time to share and exchange information. This may include using Facebook, Twitter, YouTube, Snapchat, Instagram, blogs, forums, dating “apps” and personal websites. The key element of social media… is the active nature of the dialogue, enabling user-generated content and images to be communicated instantly.”
It’s a truism to say that social media is rapidly evolving. It’s moving so fast, in fact, that some of the content in NZNO’s new guideline, updated during 2018 and published just last month, is already starting to become dated.
Part of this rapid evolution is a blurring of the distinction between social media and traditional news media. Online newspapers such as Stuff are increasingly integrating user-generated content, through a comments area, through reporting on social media posts, through embedding of tweets and Facebook Live videos directly in their articles and through an entire section dedicated to content submitted by readers, called “Stuff Nation”. For this reason, my talk will also touch on the impact of the news media.
Let me start with an immediate example – one that’s current, and close to home.
Here are a couple of photos taken earlier this month in Ōamaru.
You may recognise some of the people, and what the photos depict.
Last month, the Otago Daily Times obtained a copy of a confidential “proposal of change” document distributed to Ōamaru Hospital staff, which included a proposed staffing restructure. The proposed restructure would impact seriously on NZNO members. All current nursing positions would be disestablished. Those currently employed to fill the 35.3 full-time equivalent nursing roles would be forced to reapply for a reduced number of jobs, adding up to just 20.5 FTE.
Reflecting on the theme of today’s convention, “Nurses A Voice to Lead – Health for All”, the proposal for change could also impact on access to healthcare for the rural population inthe Waitaki District.
“The document has caused a large amount of negative discussion around the community”, reported the ODT on 25 February, “particularly on social media platforms, which has caused public unease. As a result, the Waitaki District Council-controlled company that owns and operates the hospital will hold community meetings.”
The photo on the lower left of the slide above comes from an ODT story about one of these meetings, where strong views were expressed about the proposal to cut nursing jobs. The one on the upper right, courtesy of Oamaru Captured, shows a march to support jobs and services. So here we see how social media is influencing practice environments and job security for NZNO members.
Then last Saturday, the ODT reported: “On Wednesday the Waitaki Community Hospital Action Group started an online petition on its Facebook page – Halt the Oamaru Hospital Proposal.”
That petition, fronted by former Ōamaru Nurse Manager Dr Janice Clayton, calls for a halt on the restructure because:
“The Waitaki Community deserves the right to ensure ongoing service provision at the Hospital now and well into the future.
The current staff deserve the right to voice openly what matters most to them moving forward with a new Model of Care.
Our elderly and young families deserve to know exactly how community-based and home-based care structures will affect them.”
In its first week, the petition has been signed by over 400 people – or around one in 30 of Ōamaru’s resident population.
So overall, I think the primary impact of social media on NZNO members and delegates in this instance has been to rapidly mobilise strong public support. It’s a good example of what’s known as “online-to-offline” activism, where the power of social media is harnessed to generate measurable effects in the community – in this case, to the benefit of NZNO members and delegates.
But this is not the only prominent example from this region over the last year. Here are two photos taken in the Octagon, on International Nurses Day 2018.
They depict one of 15 rallies held around New Zealand that day.
As reported in the ODT these rallies, too, were organised through social media: “A social media site has transformed into a nationwide nurses movement which will stage rallies across New Zealand this weekend”, says this article, which also carries an interview with Dunedin Hospital delegate Anne Daniels (pictured, on the right).
The site in question was the the “New Zealand, please hear our voice” Facebook group, created by two anonymous nurses after the first DHB offer was rejected. Within a fortnight, it had grown to 37,000 members.
The effect of this large social media-led campaign is probably impossible to quantify, in what was a period of intense and multi-faceted activity by and for NZNO members. But two weeks after these rallies, the DHBs lifted their pay offer to members from 6% over three years to 9.3–15.9% over 26 months. I think it’s undeniable that the impact on NZNO members was significant and positive.
But to say that the impact of social media hasn’t been universally positive would be an understatement.
I won’t dwell on this point, as I’m sure most of us who are on Facebook have plentiful first-hand experience of negative impacts, both on ourselves as members and on the reputation of our organisation. But I will refer to the end of year editorial in Kai Tiaki.
Co-editor Teresa O’Connor looked back on 2018 and reflected that, “Social media, notably Facebook, was used to mobilise nurses and to provide a platform for their views on the progress and eventual outcome of the [DHB MECA] negotiations. The power and influence of social media took some by surprise, but what was more of a shock was the rancour of many who took to Facebook to air their views.”
In this, O’Connor was echoing the sentiments of an earlier editorial by acting Manager, Nursing and Professional Services Hilary Graham-Smith, who wrote: “Some members (and non-members) took to social media to rain down abuse on NZNO and on individual staff. For many of us in the profession, that behaviour was the wellspring of deep sadness. What has the profession come to, we asked ourselves and each other as, day after day, the insults, name-calling, ill-informed commentary and blatant lies spewed forth from various Facebook pages.”
The abuse that was rained down via social media fell, above all, upon NZNO representatives in the DHB MECA negotiating team and campaign leadership. And I want to acknowledge in particular the impact this had on your local delegate, Robyn Hewlett.
In July last year, as the manifold impacts of the protracted bargaining started to mount, I called a special meeting of the Board to consider whether some organisational guidance from the governance leadership might be required. In the event, the meeting took place in August, just after the MECA offer was ratified.
One of the issues we discussedwas the impact of social media on NZNO negotiators. Afterwards, a statement penned by Vice-President Rosemary Minto was published on the official NZNO Facebook page.
It said: “The Board would like to wholeheartedly thank the NZNO negotiating team and supporting NZNO staff for their work on the recent MECA negotiations… The Board acknowledge the part that social media played in the process, which at times directed negative and personal attacks towards NZNO members and staff… The Nursing Council of NZ Code of Conduct and the NZNO Constitution and guideline on social media and the nursing profession should be considered by all nurses including NZNO members, before and during their engagement and discourse on social media sites.”
It is hard to say why NZNO experienced such a negative impact, where other professional groups taking large scale industrial action over the last year, such as doctors and teachers, did not.
One difference between NZNO and these other groups is that the others mounted high profile media campaigns, starting well before bargaining commenced, or set up their own officially moderated Facebook groups for union members to engage in online-to-offline activism.
Here on the left we see the primary teachers union launching its campaign, and on the right the creation of the secondary teachers union Facebook group, in each case six or more months prior to the start of their negotiations.
When NZNO did embark on our digital campaign on 26 March 2018, under the umbrella of #HealthNeedsNursing, it immediately generated strong positive effects for NZNO members and delegates, and for NZNO’s reputation. Although it did not utilise Facebook groups, #HealthNeedsNursing was a cross-platform, multi-media campaign, deploying text, images and video over Instagram, Facebook Pages, YouTube and Messenger.
This two-page infographic shows just how great the impact of our social media was. I have hard copies of the “Campaign at a Glance” document here, for you to take away.
Again showing the power of online-to-offline campaigning, note the three dozen rallies which were held around the country in April. Organised through Facebook Events as well as through workplaces, they involved thousands of NZNO members and supporters – even more than the numbers who took part in the #HearOurVoices marches. And of course there was integration with the historic DHB strike on 12 July. Overall, this social media activity certainly contributed to positive impacts on DHB members achievedthrough bargaining.
So far, I have offered observations and examples where social media has impacted on NZNO members collectively. I will conclude by looking at individual impacts.
Historically, nurses have tended torun into trouble on social media through breaches of patient confidentiality. The 2016 Annual Report from the Nursing Council, for example, notes that, “With the millennial generation so digitally connected, there has been concern at their reduced awareness of issues related to privacy and the increasing number of disciplinary cases related to social media.”
Patient confidentiality remains a primary focus of the new NZNO social media Guideline. But speaking with NZNO Professional Nurse Advisors in different parts of the country, new trends appear to be emerging.
Anecdotally, referrals to Nursing Council for individuals are now less frequentfor breaches of patient confidentiality, and more frequentfor social media breaches of these two standards – “treat colleagues with respect” and “maintain high standards of behaviour in your relationship with your employer”.
There is little in the way of hard data on this, as yet. The latest published Annual Report from the Nursing Council is now two years old. And I’m told that NZNO’s data collection systems, through the Member Support Centre, are not well set up to capture this emerging trend. Calls related to social media issues could be coded variously by MSC as an “Industrial – Disciplinary” matter, a “Professional –Media” issue, or something else.
But there appears to be one such case, here in this post in the “hear our voice” group in January.
“I’ve just received a message from a member who’s been reported to Nursing Council… due to being overtly savage online regarding their employer”.
I hope these personal observations and examples of social media impacts have helped to stimulate your thinking. I will leave you with one piece of advice. To avoid the negative impacts of social media for yourself and NZNO, and maximise the positive impacts, the best thing you can do is refresh your knowledge of these two guidelines.
(Following some unscripted remarks on the events in Christchurch the previous day, these were the speaking notes for my presentation.)
Photo courtesy of Kai Tiaki Nursing New Zealand.
Āta mārie, tēnei te mihi ki a koutou.
Good morning, greetings to you.
Ko wai ahau? Ko Kapukataumahaka tōku maunga, ko Ōwheo tōku awa, ko Cornwall tōku waka.
Ko te Tāngata Tiriti tōku iwi, ko Don rāua ko Helen ōku mātua. Ko Grant Brookes ahau. Nō reira, tēnā koutou katoa.
Who am I? The place I come from looks up at a mountain called Kapukataumahaka, or Mount Cargill, and sits beside a river called Ōwheo, the Water of Leith. My ancestors arrived there, in Dunedin, aboard a waka, or ship called The Cornwall. I belong to the People of the Treaty, the people who reside here under the agreement first signed at Waitangi in 1840. My parents are Don and Helen, and I am Grant Brookes.
The topic I have been given to speak about is, “Where to from here? Into the future, the path forward, what is the role for migrant nurses in NZNO?”.
Let’s begin with definitions. What is this group, the migrant nurses in NZNO? Who are they?
The answer may surprise you. We don’t entirely know.
The NZNO membership database contains a field recording a member’s “country of first qualification”. In theory, therefore, the migrant nurses in NZNO should be clearly identifiable. They would be the members who ticked a box other than “New Zealand” in their membership application, in response to this question.
However, in speaking with the NZNO Membership Department in preparation for this talk, I learnt that it’s not so simple.
Firstly, this field was added to the database only around four years ago. For members who joined prior to that, there is no record of where they first qualified. And I was told that anecdotally, the data is not reliable, as many members who have joined since 2015 left this field blank on their membership form, or filled it out incorrectly.
But when we speak of migrant nurses (and of internationally qualified health workers who may not be working as nurses, the other group covered by this conference), what we’re often thinking of are people who share particular cultural backgrounds – backgrounds other than New Zealand European or New Zealand Māori. Research suggests that the experiences of NZNO members in these minority groups (including experiences of racism) are similar, regardless of whether the person first qualified as a nurse in New Zealand or overseas.
In other words, what we’re talking about is ethnicity. And with your permission, I would like to focus on this concept, which thankfully is captured by NZNO in a time-series data set which is more robust.
Do you like data? I do, as you may have guessed. So if you’re not a fan, please indulge me for a couple of minutes as I present some charts showing the changing ethnic makeup of our membership over the last ten years.
Just one final word about data quality – up until 2015, ethnicity categories in the NZNO membership database were less specific. So, for example, members belonging to one of the many Asian ethnic groups were described as either Chinese, Indian or “Other Asian”. The NZNO Board requested refinements to the reporting categories in 2016, to make the growing diversity of our membership more visible. You will see this in the later charts. Ethnicity data captured in the NZNO database is now aligned with the fields recorded by the Nursing Council, although it’s still not perfect and anecdotal reports suggest a member’s ethnicity sometimes defaults incorrectly to NZ European.
So based on what we have, this was the picture at 31 December 2008.
Our membership was largely made up of people identifying as New Zealand European, with a significant Māori group. There was also a visible group of “Other Europeans”, reflecting the traditional trickle of migrant nurses from places like the UK and Australia.
Click on the image to play the video below and watch how it changes, year by year.
In 2010, the “Other Asian” group started to overtake “Other European”, as the primary source countries for IQNs started to change. The trend then accelerated.
And this is where we are now.
If current trends continue, New Zealand Europeans like me will be a minority of NZNO members by 2025.
It is worth mentioning in passing that there hasn’t been any similar transformation of the NZNO staff. There are almost 130 people employed by NZNO, in a variety of roles. But aside from our Chief Executive, there are still no IQNs of non-European ethnicity among them.
So that’s the picture from the last ten years. But if you go back further, the demographic transformation of the NZNO membership appears starker still. I became a member of NZNO in 2002. Back then, the organisation looked like this.
As you can see, the NZNO which I joined was largely monocultural, at least as far as our membership base was concerned.
You might also note that the opening up of this monoculturalism has come through the declining proportion of members identifying as New Zealand European. Māori membership has not declined. The proportion of members who are tāngata whenua, or people of the land, and the proportion who are tauiwi, or more recent arrivals residing here by virtue of Te Tiriti o Waitangi, is virtually unchanged through this period.
The relationship between these two groups underpins the bicultural foundation of our organisation – in accordance with the bicultural foundation of our nursing profession, and indeed of our nation. Kerri Nuku will speak more about this next.
If this is the story so far, what is the role for IQNs and migrant health workers in NZNO, into the future?
Let me first flip that question. What is my role, as Co-chair of the NZNO Board, for IQNs and migrant health workers in NZNO?
I know that as a New Zealand European, citizen and NZRN, I automatically benefit from a system of privilege, whether I like it or not. My role for IQNs and migrant health workers in NZNO is to use that privilege to make space at the top table for people without it, like you.
Your role is quite simply to take your place in the leadership of NZNO – as increasing numbers of you are already doing.
I would like to briefly showcase just a few of the leading roles being filled by migrant nurses today. Some of these people, you will probably recognise.
Victoria Santos is an IQN from the Philippines. She also holds a senior leadership position in the governance of NZNO. Victoria sits on the Membership Committee, the national body which advises the NZNO Board of Directors on the views and needs of the diverse membership. The Membership Committee also helps to carry out delegated work such as drafting the constitutional changes which will this year see voting on NZNO policies and rules opened up to everyone, though an online “one member, one vote” system.
Jed Montayre is also from the Philippines. Within NZNO, Jed is an elected member of the National Committees of Gerontology Section and also the Nursing Research Section. He has served on the abstracts committee which selected the papers for presentation at the NZNO Annual Conference. Here, he is pictured receiving the award as joint winner of the NZNO Young Nurse of the Year in 2016.
One of the three abstracts chosen for last year’s NZNO Annual Conference was on “The Experience of Migrant Health Workers in New Zealand”. It was jointly presented by three Filipinos – Joey Domdom, Judith Salamat and Mayie Pagalilauan – in conjunction with Toga Katyamaenza, an IQN from Zimbabwe. Here they are pictured with IQN and former NZNO Board member Monina Hernandez, who will speak to us later this morning.
Shamim Chagani is an IQN from Pakistan, and an elected member of the National Committee for NZNO Nurse Managers New Zealand. She is also the editor of the Nurse Managers’ newsletter, Te Wheke, a Māori title which means, “The Octopus”.
But IQNs are not just demonstrating professional leadership within NZNO.
This poster features Ebson Abraham, an IQN from India. The poster was produced by the NZNO Tai Tokerau Regional Council for International Nurses Day last year, to celebrate local NZNO leadership in Northland. The writing is probably too small for you to read, but it says Ebson was a workplace delegate at Cairnfield House Rest Home in Whangarei, where “he took responsibility for NZNO services, promoting the union movement from scratch and then constructed a movement that is measurable by the increase of NZNO membership density up to 80% that eventually built a strong force for change. This wave became a pillar… for NZNO bargaining in 2016/17 with an effective settlement of a collective agreement in 2017”.
As an aside, there is a widespread assumption among New Zealanders that union membership and activism are somehow foreign to the cultural values in the primary source countries for IQNs today.
The diversity clearly displayed on marches and rallies by DHB nurses last year should help to dispel that stereotype. But so would greater knowledge of overseas nursing unions, which are growing under very difficult conditions and waging struggles on a scale and intensity which make our DHB strike look timid.
A case in point is the United Nurses Association of India. It was formed in the southern state of Kerala in 2011, in response to the suicide of a nurse who had been bullied by her managers. It now numbers over half a million members. Months of protests and strikes in 2017 and 2018 won agreements on pay rises for around 80,000 nurses in private hospitals. At one hospital in Kerala, nurses remained on strike and picketed outside the facility daily, for over a year.
The spectacular rise of the United Nurses Association is an amazing story. I hope to meet leaders of that union for the first time in July at the annual meeting of our international union federation, Global Nurses United. But it’s by no means an isolated case. Nurses in the Philippines have been organising for decades – again under very difficult conditions – through unions including the Alliance of Health Workers and more recently through Filipino Nurses United. Last year, Kerri Nuku and I attended 61st annual general meeting of the Fijian Nursing Association. FNA has been active as a Pacific nursing union since 1977, including campaigning for workers’ rights under military rule, and so on.
Returning to the slides, the last two IQN leaders in NZNO I wish to showcase highlight the need to avoid assumptions when it comes to migrant nurses.
Current Board member Eseta Finau occupies the highest leadership role in NZNO of any IQN. She will talk to us shortly about that role. Despite also being the most Tongan person I know, however, she actually qualified as a nurse in Australia. Gidday cobber!
And then there are NZNO leaders who you might not pick as IQNs from their appearance.
Debbie O’Donoghue is a former NZNO Board member who now serves on the national committee of NZNO Nurse Managers New Zealand. She is also an IQN, from the UK.
But leadership for IQNs within NZNO does not depend on holding a title, like these people. The NZNO Strategy for Nursing 2018-2023 recognises that, “Many nurses demonstrate excellent… leadership, though they may not recognise this, associating leadership only with formal roles.”
In many ways, leadership exercised by people without a formal title is the most important kind. As Bernie Sanders likes to say, “Real change does not happen from the top down. It happens from the bottom up.”
One of the ways that any member can influence NZNO’s direction from the bottom up is by responding to consultation requests. This is where staff from the NZNO policy and research team seek member input, in order to determine NZNO’s position on a wide range of issues. They do this by emailing all member groups, including Regional Councils, to ask for feedback.
They also post the requests on the NZNO website, under the menu “Get Involved > Consultation”. If migrant nurses are not getting the consultation requests by email, from a member group, you can sign up on the website to be notified each time a new one comes out.
Here is a recent request, asking for input to shape NZNO’s view about the changes to temporary work visas for migrants currently being proposed by the government. Unfortunately, the deadline has passed for people to respond to this request, although if anyone is interested in making an individual submission to the government, you can do it via the MBIE website until Monday, at the address on screen.
So these are some of the ways that migrant nurses can take up your role as leaders of NZNO and use your power to make a difference.
But as the title of Monina Hernandez’s presentation on today’s programme reminds us, the role for migrant nurses in NZNO is not just about “making a difference”. It’s also about “being yourself”. I will end on this point.
Coming up before morning tea is Abel Smith’s presentation, “An introduction to the Pacific Nursing Section”. The PNS is one of NZNO’s 20 colleges and sections. I am really looking forward to it because for me, this group epitomises what it means for ethnic minority members to be themselves while also making a difference.
NZNO sections and colleges are groups of members with a focus on a specific field of nursing. The colleges are groups relating to a specific clinical specialty, while the sections are groups representing a role or membership classification, such as those sharing a specific culture or cultures. Formed in 2008, the Pacific Nursing Section was the last NZNO section to be established before a moratorium was placed on the formation of new sections in 2011.
The NZNO Constitution was amended last year, through a remit submitted to the NZNO AGM by the Greater Auckland Regional Council, to lift the moratorium and allow the creation of new colleges and sections.
The rationale provided in support of the remit noted that: “NZNO structures need to be flexible enough to respond to the changing reality”. And we’ve seen in the pie charts the changing reality of NZNO membership. The remit rationale added: “Various membership and role classification groups exist without a corresponding NZNO structure to date. Examples include… internationally qualified nurses”.
I will now hand over to Kerri Nuku. Because we will be back as part of the discussion panel after lunch, and because I have used up all of my available time, I would ask that you save any questions until then.
Titiro ki muri kia whakatika ā mua. Look to the past to proceed with the future.
I CAME across this proverb last month at Te Matatini, the national kapa haka championships in Wellington. It summed up for me our task as we prepare to update and replace NZNO’s five-year strategic plan, which expires next year. The process approved by the board will involve input from external stakeholders, NZNO staff and members.
Looking back, and thinking about the future, gives us all a chance to re-focus on the big questions for NZNO. Who are we here for? What are we hoping to achieve? How will we get there? What’s going on in our environment – political, economic, social/cultural, technological, legal and environmental – that we will need to respond to?
Much has changed since delegates at the 2015 NZNO annual general meeting voted to approve the current strategic plan. Back then, as chief executive Memo Musa reminded us, union membership was declining. Law changes had made it harder for unions to operate, and union influence was dwindling. An NZNO strategy stressing nursing professionalism fitted with the times.
Fast forward to 2019 – anti-union laws have been reversed, and the trend of declining union membership has also turned around. Union engagement with employers and government is stronger. Health funding is no longer falling. There’s also much to learn from last year’s unprecedented DHB MECA campaign.
The board has also agreed in principle on a review of our operational structures, to make sure they’re suitable for implementing the new strategy. And while no decision has been made, we have discussed whether the NZNO constitution – which spells out who has the power to do what in NZNO, and members’ rights and responsibilities – might need to be reviewed, as well.
Who are we here for?
In my view, the answer to the first big question, “Who are we here for?”, is that NZNO is here, above all, for the members, and we must keep members at the centre of our planning. If we focus on supporting and empowering members, then our strategic goals and the ways to achieve them will become clear.
Members see the impacts of health and social policies, and belong to communities who experience impacts, too. Supporting members means our strategic goals should include political changes.
All of us are unionised workers and health professionals. Focusing on members solves the conundrum of whether to stress “industrial or professional” strategies. At all times, we are both.
And nurses and midwives are required to practise in a culturally safe manner, under the Treaty of Waitangi/Te Tiriti o Waitangi. Supporting members means strengthening biculturalism.
Such a member-centric strategic plan might suit an NZNO structure where more authority and resources are devolved to our volunteer member-leaders.
It could drive full implementation of NZNO’s organising model, an approach which empowers members in the workplace to act as a team in their own interest, rather than just looking to an NZNO staff member to “fix” things for them. •
First published in Kai Tiaki Nursing New Zealand, March 2019